

TOPICS
For those new to this issue it’s best to know these terms before reading.
4) Affirmative model mental health professionals & doctors & statements suggesting lack of concrete knowledge of long-term safety & effects on desistance
While trans activists are well within their right to advocate for what they believe is best for their community, social scientists, counselors and doctors are ethically and legally bound to base their care on evidence. Very early social transitions and surgery on minors are happening because of some early positive but limited research (de Vries 2014), (Olson 2016). Doctors and therapists have a right to discuss the positives of these studies and disseminate that information to the public. However, statements from some doctors and therapists go beyond what they know about youth social and medical transition. In addition, clinicians sometimes seem to demonstrate a lack of concern that new protocols may create false positives, or actively encourage youth to identify as transgender, or promote unfalsifiable arguments, which could open themselves up to litigation by admitting they do not know the consequences of their actions.
A. Statements admitting trans health care professionals are socially and medically experimenting on their patients
Doctors and therapists who approve of early medical transition support policies such as starting hormone blockers as young as ten and reducing age limits on cross-sex hormones and surgery. They have made numerous statements indicating they do not know the ultimate consequences their protocols will have on minors. This would mean these children and teens are currently medical experimentation subjects. This is interesting because designing a study with a control group (where trans youth are given emotional support and supported in their gender nonconformity while being offered less physically invasive coping strategies than drugs and surgeries) is considered unethical and “conversion therapy.” Yet some statements indicate that medically experimenting on minors by drugging them, sterilizing them, and stunting the development of their sex organs while not knowing if the youth will remain trans is considered morally acceptable.
Endocrinologist Dr. Norman Spack who questions delaying cross-sex hormones says:
“There is no consensus among mental health professionals regarding appropriate intervention, or even appropriate goals of intervention, for children diagnosed with GID”
From the Tavistock gender clinic in Britain:
Dr Bernadette Wren, head of psychology at the Tavistock, doesn’t claim to know all the answers. The field of gender identity is so new and fast evolving, she says, “I just have to be really honest and say at the moment we don’t have a way of understanding it completely.”
Dr. Rob Garofalo tells PBS:
There are so many unanswered questions around the long-term consequences, and whether your health risk profile really becomes that of a male or female,” Garofalo says. “If we start testosterone today, will you have the cardiac risk profile of a male or female as you grow older? Will you develop breast cancer because we’re administering estrogen?
And:
I think those are the unanswered questions that really trouble me and can only be answered with long-term follow-up studies.
And:
“The stakes are super high, and we don’t have all the answers,” Garofalo says. “Hopefully, there’s going to be more research and some of those unanswered questions, hopefully, will begin to be answered.”
Stephen Rosenthal in Endocrinology Today admits he is experimenting on his patients:

One critical issue at this point in time is that none of the options for pubertal blockers on the market are FDA approved for transgender use. No pharmaceutical company has taken the steps necessary to change their labelling to include this category.
Endocrinologist Dr. Johanna Olson-Kennedy (Gender Odyssey, 2017):
We don’t have enough data to know (about testosterone). It’s just all over the place right now. And so, I think once we have a better idea of that or we collect all of this data together, we are going to say “Hey, it turns out if you’re within a certain amount of time of menarche you can induce a male growth spurt, then we will probably make different decisions around testosterone and blockers.
In light of uncertainties, Johanna Olson-Kennedy states that female youth who may regret their double mastectomies can just “go and get them [new breasts] later.”
Examples of youth who have had sexual function impaired can be found in this section. Here are several other quotes from Johanna Olson-Kennedy where she seems to indicate her protocols may be permanently destroying the sexual function of dysphoric males who choose this path as young as 11 years old:

WPATH Facebook page March 18, 2016
There are multiple issues with the above statement:
1) The doctors involved are applying a technique that permanently alters the youth’s genitals, which in some cases appear to become “NON FUNCTIONING,” raising the question: can an 11-year-old, who has never even explored their sexuality, consent to permanently eradicating their sexual function (possibly for life)?
2) It appears these consequences are an afterthought and not seriously considered before this protocol was implemented. This seems to raise legal issues, especially if the reality of “micro penis,” sexual function consequences, and surgical consequences were not fully disclosed to the youth or the youth’s parents (what this doctor has disclosed to parents is not known here).
3) Doctors are eliminating choices about what types of surgeries trans youth may or may not wish to have later. Many MtFs do not get bottom surgery, and not all MtFs are dysphoric about their lower bodies. Nor does lack of bottom surgery preclude MtFs from finding partners.
4) It’s tragic that these young people view their lives as “on hold” and that moving forward with life is wholly dependent on surgery. There should be an ongoing discussion about how dysphoric youth can best be supported by the mental health community, their families, and the culture, with alternative ways to cope with dysphoria. This may be especially helpful since “shifting dysphoria” and viewing transition are issues in the trans community.
Dr. Olson-Kennedy has made similar statements about this topic. These side effects were possibly a secondary concern to stopping sex characteristics from developing naturally.
Gender Odyssey, 2017:
So how many people here saw the episode of Jazz Jennings? For people with testicles who are blocked at tanner stage 2, they do not have a lot of penile tissue and when you do a procedure that you use the tissue of the penis to make a neovagina…usually you would just do an inversion and use that tissue but if you don’t have a lot you need to do graft from another part of the body, usually scrotal tissue. There are other ways that people do this, does not preclude you from having a vaginoplasty, but people need to think about this. Blocking is one tool that’s awesome for a lot of people. And what does that mean? Does that mean that trans feminine, trans girls who get blocked in tanner 2, we are making the assumption that all of them are going to have genital surgery? Are we doing that? (Laughs nervously) I’m just saying we might be doing that. And so that actually is worthy of a conversation. Because many trans women do not have genital surgery they love their genitals, enjoy their genitals, like to use them. That’s fantastic.
We love people who love their bodies and use them and enjoy them. That’s a great human place to be. But we have to ask ourselves if you have tanner 2 male genitals are you going to be able to use them, are you going to want to be able to use them? Or are we just assuming that everybody is now going to have to say ‘Well I either need to go through puberty to get adult sized genitals or I’m going to have these genitals that I have or I’m getting surgery.’ Does that make sense? If we are judging the success of vaginoplasty by post-surgical orgasm how do we know people are having orgasms prior to surgery if we are blocking them at tanner 2.
Another quote indicates doctors need to collect data on what are now medical experimentation on children to determine what numbers of them will lack sexual function in the future (WPATH Facebook page March 19, 2016):
I hope that providers are discussing masturbation and orgasm with their patients around the time they are starting hormones. I certainly do because if we are to measure the success of post op procedures by orgasm potential and people have no experience of pre-op orgasm or other or other sexual experience we are failing.
Western society is moving towards an affirmative model where decisions made by 11-year-old children to sterilize themselves and risk losing sexual function to “pass” better are seen as worth it. Below is a further discussion by WPATH members indicating the potential for damage to sexual function:
WPATH Facebook
An apparent lack of foresight may have happened regarding the parents of Jazz Jennings, whose parents seemed surprised when the doctor told them their child did not have enough tissue to do the “gold standard” vaginoplasty. Did doctors not fully inform the patient and parents of all the consequences of an early social and medical transition? Jazz has had severe complications from surgery and may never experience fully functioning sexuality.
Kristina Olson (no relation to the above doctor) and Lily Durwood, researchers from the University of Washington involved in the Trans Youth Project, admit social transitions are an experiment. However, they appear to view this as more of a positive that will ultimately help trans youth. In this piece for Slate, they call parents socially transitioning their very young children “pioneers” and describe concerns that early social transition may increase persistence as “alarmist”:
From a scientific perspective, we are fortunate that today there are larger numbers of children who have socially transitioned, who can be followed to assess rates of regret and the social or psychological costs (or benefits) of “de-transitioning”—some of the many goals of our ongoing study.
There are several issues with this quote:
1) This is all being done without a control group. Obtaining an accurate picture of the consequences of children living as trans from age five to 10, where they will most likely go on hormone blockers as young as nine, will not be possible. Furthermore, it is impossible to track accurate “regret rates” involving decisions made by a 10-year-old who never experienced natural puberty, as they will be unable to compare their outcome to what may have been.
2) There seems to be no worry that social transitions may create false positives. This is odd as the possible results are sterilization, castration, and sexual dysfunction perpetrated on a biologically healthy body. Dr. Ken Zucker, one of the most experienced doctors in working with trans youth (and despised by many activists for his cautious approach), believes early social transitions will track at least some desisters into medical treatment. While we don’t support the behavior modification techniques that were reportedly used in his clinic, other clinicians share this concern (Dr. Wren and Dr. Carmichael and, more recently, others in Britain and Finland (in English)). This is not emphasized in the article.
3) They put “detransitioning” in quotation marks. The reason these researchers chose to do this is unknown. But it is likely because it is considered transphobic to even discuss detransition in some affirmative model circles and the transgender conferences (Gender Odyssey, WPATH) researchers attend (see here and here). Trans activists (such as Julia Serrano and others) also promote the narrative that people don’t detransition because they do not want to be trans anymore, or in some cases have accepted a male or lesbian/bi female identity, but because of trans oppression. This politically motivated claim expresses bias that scientific researchers should not hold. “Detransition” is a real event that happens to some people; it is not a theoretical concept that belongs in quotes. Some detransitioners greatly resent (see here and here) the dismissiveness among trans activists and some psychologists about their experiences.
There is no current consensus that the affirmative model supports the psychological process that helps a child desist or children’s long-term physical health.
Dr. Wren from the Tavistock gender clinic:
Wren said future generations might condemn the way such children were being handled: “Of course you have to think that in another generation we will have done something which is not regarded as having been wise.” She also acknowledged that some youngsters could regret their decision to change gender when they grow up and that there were risks involved, including the loss of the ability to have children, particularly for those born as boys.
“Perhaps the choices they make when they are 16 look different when they are 30,” said Wren, speaking in advance of a conference next month about improving support for children who question their gender. “You can accept their feeling about gender difference but you do have to say alongside that — and without being transphobic — that there are really difficult treatment choices to be made.
B. Adult professional influence on trans identification in minors
Body modifications involved in gender transition are extreme. A youth cannot fully absorb the consequences of this until their mid-twenties, and the reality is some youth desist. Because of this, it is worth questioning if therapists and doctors may be asking their patients leading questions. This appears to be happening.
Here, Dr. Johanna Olson-Kennedy provides an example of a youth who did not express distress about her gender, identifying as trans after a visit with her.
USPATH conference in Los Angeles in 2017:
Olson’s spouse, Aydin Olson-Kennedy, a social worker in gender identity and an FtM trans activist says “you have to hear the Pop-Tart story real quick.” Audio here
(J. Olson) An 8-year-old kid comes into my practice, and this is the story with this kid: Assigned female at birth, 8 years old, was completely presenting male whatever that means—short haircut, boy’s clothes–but what was happening, is, this kid went to a very religious school and in the girls’ bathroom which is where this kid was going. People are like, “why is there a boy in the girl’s bathroom? That’s a real problem.” And so, this kid was like, so that’s not super working for me, so I think that I wanna maybe enroll in school as a boy. This kid had come up with this entirely on their own.
When the kid came in, mom was like, “oh we don’t know what to do, so please help us” and so we started talking about it and what was interesting is that …you know some kids come in and they have great clarity and great articulation [sic] about their gender. They are just endorsing it, “this is who I am, and yes there’s gender confusion but it’s all of you who are confused,” so there are those kids. So this kid had not really organized or thought about all these different possibilities.
You know the mom had shared this whole history, and said, when the kid was 3, the kid said, “Could you stroll me back up to God so I can come back down as a boy” and the kid’s like,” Ah, I didn’t say that.” You know, 8-year-olds, so I’m like, ‘I don’t think your mom made that up, that’s crazy.’
So, at one point, I said to the kid, “so do you think that you’re a girl or a boy? And this kid was like…I could just see, there was, like, this confusion on the kid’s face. Like, “actually I never really thought about that.”And so this kid said, ‘well, I’m a girl, ’cause I have this body’. Right? This is how this kid had learned to talk about their gender…that it’s based on their body.And I said, ‘oh, so,’ and I completely made this up on the spot, by the way, but I said, ‘Do you ever eat pop tarts?’ And the kid was like, ‘oh, of course.’ And I said, ‘well you know how they come in that foil packet?’ Yes. ‘Well, what if there was a strawberry Pop-Tart in a foil packet, in a box that said Cinnamon Pop Tarts. Is it a strawberry pop tart, or a cinnamon pop tart?’ The kid’s like, “Duh! A strawberry Pop-Tart.” And I was like, ‘so?’ And the kid turned to the mom and said, “I think I’m a boy and the girl’s covering me up.”And the best thing was that the mom was like, (happy reaction) and she goes and gives the kid a big hug and it was an amazing experience. But I worry about when we say things like “I am a” vs “I wish I were” because I think there are so many things that contextually happen for people in around the way they understand and language/ gender. So, I don’t think I made this kid a boy. “I don’t THINK so. I mean, and if I did, and I’m wrong, then I’m totally gonna come to this conference and tell people that I was wrong. I will. But I think giving this kid the language to talk about his gender was really important. And actually, it did not make him a boy, it gave him language to understand his gender.
Children expressing extreme dysphoria need help and support. However, this youth was not expressing gender discomfort, and this scenario seems to go beyond the stated goals of the affirmative model. There are several issues with Olson-Kennedy’s behavior from the perspective of people who are concerned about early social transition and hormone blocker use:
1) Even some strongly dysphoric youth desist, and this youth was not expressing gender dysphoria. Why did this child need to be questioned about her gender?
2) There is a strong association between homosexuality and childhood gender-nonconforming behavior, and there is evidence homophobic bullying increases trans identification. Many people worry about borderline pre-gay and lesbian children under the affirmative model. Some LGB people claim early gender transitions are something similar to “eugenics.” Examples like this promote a culture contrary to accepting gender nonconformity and one’s body. The practice encourages youth to dissociate from their body, where the next step is to correct their gender expression with hormone blockers, cross-sex hormones, and surgery at ages when they are too young to comprehend the consequences fully. Children are very aware of gender expectations and are influenced by gender stereotypes. They are not in a position to understand their sexual orientation or their ability to break social norms at young ages. The intent of this may not be homophobia or anti-tomboy, but the concern is the effect could cause harm and confusion to gender-nonconforming children. Some LGB people view this as a form of anti-LGB activism, whether this is the intention of liberal-minded doctors or not.
Advocates of the gender affirmation model view not affirming a trans youth’s identity and not providing immediate medical treatment as psychologically damaging to them, which may be true. Medical transition may or may not be worth the downsides to those youths. But suggesting to borderline dysphoric gay and lesbian young people that they could be trans because they are gender nonconforming can be harmful to them.
3) Questioning transness in a young girl who is not insisting she is a boy is gender stereotyping and may encourage gender non-conforming boys or girls to see themselves as trans. This may influence not only lesbian or bisexual tomboys but also heterosexual girls who come to view themselves wrongly as male. This may confuse them and their gender identity and sexual orientation development. Two girls who identified as heterosexual did have difficulty adjusting back to their roles as girls after social transition in Steensma (2011):
Given our findings that some girls, who were almost (but not even entirely) living as boys in their childhood years, experienced great trouble when they wanted to return to the female gender role, we believe that parents and caregivers should fully realize the unpredictability of their child’s psychosexual outcome…They may help their child to handle their gender variance in a supportive way, but without taking social steps long before puberty, which are hard to reverse.
4) There are decades of research in developmental psychology showing young people are heavily influenced by their environment, peers and adults’ opinions. The above example shows an authority figure signaling to the child she thinks her tomboyishness may be transgenderism. Children are susceptible to adult reinforcement, especially if the adult is their doctor or teacher.
The position of GHQ is that doctors and therapists should not make comments to encourage trans identification in minors because they are gender nonconforming or gay or lesbian. And that medical treatment should be a last resort, not encouraged. (see Viewpoints and Mission).
5) There is much information on social contagion and body dysmorphia in young females, and there are significant increases currently in trans-identified females. It appears young females can be susceptible to suggestibility, and social contagion fuels body dissatisfaction in tween and teen girls. The social environment can strongly affect young female psychology, as seen in many examples of mass psychogenic contagions. Trans identification in tween, teen, and young adult females has skyrocketed in the last five years.
6) The influence of hormone blockers on gender identity development is unknown. The youth in this example will likely be put on hormone blockers as that is the protocol now that she identifies as a boy.
7) Many promoters of the gender affirmative model, to assuage public concern, claim they are only socially transitioning children who are “truly trans” who are “insistent, persistent, and consistent” and say they are the opposite sex. The narrative is that tomboys and “girly” boys who are just gender nonconforming are not affected. But this is not the case, as seen by a doctor from one of the largest gender clinics in the country (Children’s Hospital, Los Angeles).
Examples of harm to teenagers from being targeted because they are gender nonconforming or from doctors who enthusiastically encouraged a trans identification already exist. It is potentially harmful to gender-nonconforming children who look to adults for their understanding of the world and of their gender specifically. There have been doctors whose patients included teens who have had governmental investigations/legal action taken against them for the overzealous transitioning of minors. Dr. Reid and Dr. Curtis in Britain are two examples.
was found to have repeatedly breached guidelines set by the Harry Benjamin International Gender Dysphoria Association, regarded as the minimum standards for the treatment of transsexuals.”
In the case of Dr. Curtis, who took over Reid’s practice and is a member of WPATH:
One of the most serious cases concerns a female patient who regrets switching to a male role. She underwent hormone treatment and had her breasts removed. The woman is one of the complainants in the current GMC investigation. Other cases include patients who were allegedly prescribed hormones at age 16.
Below is an account of a mother who claims her child was actively encouraged to adopt a trans identity by a school counselor. She says the school then hid the fact that the child was identifying as trans from the parents. This letter was written to the public health department at Brown University in response to them removing a link to a study trans activists did not like.
My family’s experience is not anecdotal, nor are we “right wing.” Our 15-year-old child had no gender nonconforming history before spending nine of the last twelve months believing she was “really” a man, simply because when she asked a counselor about kids at school becoming “trans,” that counselor--without any evidence or investigation, and with total disregard to a history of traumatic brain injury and other mitigating factors--suggested that wondering about trans things means you're probably trans.Our family would not have known this was the content of their sessions if not for a smart-phone glitch sending us texts from the therapist intended for our child. The therapist was fired immediately and our original care team brought in to deal with the real issues. Within weeks our child stopped believing she was “really a man” and was immensely relieved.
But, had it not been for the smart-phone glitch, my daughter could have been put on testosterone and had a double mastectomy within weeks, without my consent or knowledge, due to my state’s 15-year age of medical consent and very active trans lobby willing to provide funding and drugs, no questions asked.
The picture below (see this video 3:07:00) is of a gender workshop in a California school put on by Gender Spectrum. This organization is part of the Child and Adolescent Gender Clinic (CAGC) at UCSF Benioff Children’s Hospital. Diane Ehrensaft, one of the most ardent promoters of the affirmation model and a strong advocate for early gender transitions and early medical interventions, is a board member. Joel Baum, director of education and training for Gender Spectrum, is also the director of advocacy for the CAGC.
Here, 5th graders are encouraged to see their personality traits as being related to gender stereotypes and to view themselves as transgender. This may or may not have been the intention, yet it appears to be the result of the exercise. In the below picture, children are dissociating from identification with their biological sex even though 15 years ago, transgenderism was very rare in the population. The image below reinforces the concept that gender identity is hard-wired, innate, and not prone to outside social reinforcement. It’s not plausible to argue most of these children would identify themselves on a transgender spectrum two decades ago. This indicates social effects of gender ideology on young people.

While androgynous men and women have always existed, especially in the gay and lesbian community, what is new in the “LGBTQ” youth population is a culture of intense focus on pronouns to the point of experiencing anxiety and anger if “third gender” pronouns are not used. Whether or not this is healthy is explored further in the section on the cultural ripple effects of gender ideology. It is worth asking if this identity is being induced in gender-nonconforming children and encouraged by the culture and adults around them.
Below, Diane Ehrensaft explains “non-binary” dysphoria:
Another group who may be at risk if they socially transition are those children whose gender identity is outside of the boy/girl binary (e.g., nonbinary, bigender, gender fluid, and agender). For example, they may refer to themselves as a “girl-boy” or having no gender at all. The level of dysphoria for these children can be as profound as for other transgender children who identify with a binary gender. They may request gender neutral pronouns or no pronouns at all. These children often present as persistent, insistent, and consistent as those children asserting a binary transgender identity. Socially transitioning for these children is blending gender in ways that often makes people around them, parents, teachers, peers, etc., very uncomfortable, especially if they were assigned male at birth. They are at increased risk of bullying, physical violence, and ostracism (Greytak, Kosciw, & Diaz, 2009).
Parents may insist that they have to either be a boy or a girl, or believe it is a phase on the way to some other identity. Without language to describe themselves or acknowledgment of their congruent pronouns and asserted identity they are rendered invisible (Giammattei, 2015). If they move fluidly between different expressions of gender, others are likely to assume their current presentation is who they are, especially if on that day it is aligned with their sex assigned at birth. For these children, this can make them feel invalidated at every turn. These children are most at risk for negative mental and physical health risks in communities that do not tolerate gender diversity.
While pre-gay and lesbian youth have always expressed gender nonconformity and sometimes struggled with gender dysphoria, there is no historical evidence of people experiencing feelings of invalidation, anxiety, and bitterness because society refused to recognize them as “no gender,” “bigender” or “agender,” with use of self-created 3rd gender pronouns. This is a new way dysphoria is expressing itself, and it is increasing.
One reason to question this can be found in a quote by Kristina Olson at Gender Odyssey in 2017. Kristina Olson indicates young children have no concept of a third gender when they are small. The context of this quote is that another student, planning on being a mental health professional (who identifies as non-binary herself), asks how they can improve identifying “non-binary” children (Gender Odyssey, 2017):
It turns out one of the biggest stumbling blocks to creating non-binary measures is that, that very young kids it’s hard to explain, um so it’s a lot easier actually with adults, um older teens, who actually think about gender much differently than a just a generation before. I think young kids to get them to truly understand something beyond boy girl, or like a little boy or a little girl, um is pretty challenging.
This comment indicates that there aren’t really “non-binary” young children. Is non-binary identity innate or not? It’s likely culturally influenced and encouraged in gender-affirming environments. According to Olson’s comment, gender wasn’t looked at like this in the past (“it’s hard to explain, um, so it’s a lot easier actually with adults, um, older teens, who actually think about gender much differently than a just a generation before”).
Claims that there is an innate need for a child, or even an adult, to be called a third-gender pronoun or risk emotional damage should be treated with skepticism. There are no reports from the past from PFLAG (the organization that would be helping parents deal with gender nonconforming effeminate gay boys) that these youths experience anxiety and anger because they could not be a “no gender.” Individuals in the gay and lesbian community have always played with gender nonconformity in a way that did not necessitate imposing special language or treatment by society. There is a tiny minority of cultures who have alternative pronouns for reasons we don’t understand. Some cultures in the past may have recognized gender-nonconforming people as being “different.” But they often were cultures that had strict separation of labor and social roles between men and women. This is not nearly as much of an issue in the modern West, where men and women are generally allowed (except in some work settings) to choose their dress, jobs, and personal expression.
It’s also relevant to look at the culture the affirmative model movement is creating, as exemplified at these gender conferences now that Ph.D. students are motivated to “identify” and diagnose “non-binary children.” This is ideological indoctrination and not truly “letting the child lead,” a phrase affirmation model advocates often use.
Gender Odyssey:
You mentioned earlier that you’re going to be developing measures about the non-binary kids. Are those going to be in addition to the gender measure that you mentioned previously?...Because I’m actually a doc student up in social work right now and I’m non-binary and thinking back about how I was at that age the measures you mentioned earlier, I don’t think I would’ve been captured as a non-binary person or a trans person. And thinking about the teenagers I’ve worked with I wonder what their experience would be and it’s really like, really difficult to capture the nuance between gender identity versus gender expression.
3rd gender pronouns and the need for them are controversial even within the LGB and T populations. It’s also interesting to note that “gender expression” is almost always heavily dependent on gender stereotypes.
C. Unsubstantiated claims: it is known that social transitions are “fully reversible”
In the past, mental health professionals would try to get children and adults with gender dysphoria to accept their biological sex, sometimes in harsh and unsupportive ways, and with little success in older teens and adults. With increased understanding, the more recent model at gender clinics has been “watchful waiting” or “the Dutch model” (the Dutch have been trans research pioneers and recommend this approach). In this model, parents support the child’s gender nonconformity but don’t necessarily validate their cross-sex identity, as it may change. Full affirmation and social transition are increasingly recommended, particularly in the United States. However, due to the reality that some youth outgrow GD, this is not supported by all gender experts.
A review of the information on gender dysphoric children and the numbers of children who outgrow GD (desist) can be found here. Below are quotes from a study confirming the phenomenon of children aligning with their biological sex even after experiencing significant gender dysphoria:
Multiple longitudinal studies provide evidence that gender-atypical behavior in childhood often leads to a homosexual orientation in adulthood, but only in 2.5% to 20% of cases to a persistent gender identity disorder (3, 6, 22). Even among children who manifest a major degree of discomfort with their own sex, including an aversion to their own genitalia (GID in the strict sense), only a minority go on to an irreversible development of transsexualism (6).Irreversibility of the manifestations, however, is considered to be an indispensable requirement before the diagnosis of transsexualism can be made, or any body-altering treatments initiated. In England and Canada, in accordance with this view, hormonal treatment or surgery is not recommended until the patient's somatic and psychosexual development is completed.
And:
Of children with even severe gender dysphoria and cross-sex identification, about 85% do not develop a persistent transsexual identity in adolescence… Reliable indicators are not so far available regarding which gender dysphoric children cease to be so in puberty and who develop transsexual identity.
And a quote from “Desisting and persisting gender dysphoria after childhood: A qualitative follow-up study – Review”:
There were no differences in childhood behavior between the group that lost their gender dysphoria and the group that did not.
Given this information and what we know about cultural and parental influences on child development, it seems like social or medical scientists should ask: what psychological effects come from socially transitioning a 5-year-old child? How does early social transition affect the possibility of desistance? Discussion around these questions appears lacking (at least publicly) among pro-early social transition and medical transition health professionals. Some statements made by gender professionals possibly indicate a sense the question is irrelevant to them or even transphobic. What evidence do they have that a child living as the opposite sex from age 5-11, crucial years to the child’s mental and social development, has no impact on their self-perception around their gender and does not affect the gender alignment process many children experience according to all research?
Multiple statements on the “reversibility” of an gender social transition
Below are just a few examples of health professionals stating social transitions are fully reversible:
Johanna Olson-Kennedy: “Social transition is a reversible intervention. It is %100 reversible.” (USPATH, 2017).
AAP.org: “If the child or family later realizes the need to transition back to the birth gender, that can also happen, with the appropriate social supports and without any irreversible changes.” For a critique of the AAP’s flawed policy statement see here. Many other mental health, medical health, and “LGBT” organizations describe social transition as “fully reversible.”
Dr. Jennifer Hastings “So, what do you think, clothing, social transition, hair, is that irreversible? No, that is completely reversible.” (3:36:29-3:46:41)
Michelle Forcier claims social transitions are fully reversible in an NBC interview, “And it’s reversible, if for some reason somebody says “oops I was wrong,” which most of these kids never do, they can continue back in the assigned birth gender.” (5:38-5:53)
K. Olson and Durwood (directors of the Trans Youth Project) make the following claim in this 2016 published study. Interestingly, desistance is not mentioned even once in this article, which begs the question: is desistance irrelevant?
More striking to many, a large number of these children have “socially transitioned”: they are being raised and are presenting to others as their gender identity rather than their natal sex,1–4 a reversible nonmedical intervention that involves changing the pronouns used to describe a child, as well as his or her name and (typically) hair length and clothing.
In this piece for Slate, the same researchers address public concern for transitioning young children and respond to a critical article:
First, and most critically, the only intervention that is being made with prepubescent transgender children is a social, reversible, non-medical one—allowing a child to change pronouns, hairstyles, clothes, and a first name in everyday life. No one in mainstream medicine (or elsewhere, to our knowledge) is performing surgery on or providing hormones to prepubescent transgender children.
The surgery comment is a moot point. There would be no need to perform surgery on prepubescent children. And the process of medicalizing the child (by putting them on Lupron or other hormone blockers) starts as young as eight in females and eleven in males.
In another quote, they address neuroscientist and journalist Debra Soh’s concerns that social transition may increase persistence of gender dysphoria in pre-gay youth:
“Thus, sentences such as Soh’s, “We don’t allow children to vote or get tattoos, yet in the name of progressive thinking we are allowing them to choose serious biomedical interventions with permanent and irreversible results” are simply irrelevant to the discussion of social transitions and prepubescent children…Large numbers of transgender adults do not pursue these medical interventions, and we have met adolescents, even ones who have socially transitioned before puberty, who are making that same decision. So even the argument that allowing early social transitions will lead to an inevitable use of hormones and surgery is misleading.
Kristina Olson, Lily Durwood, and others support the early social transition of dysphoric children. However, they cannot cite any research that indicates a child living the majority of their life as the opposite sex, through critical times of brain development and social development, will easily be able to change their minds. They do not know what the effect will be on a dysphoric female child who is validated as male her whole childhood, who attends support groups—some of which are extremely pro-medical transition and very politicized environments— where she and all the other children are validated as trans. They do not know the effect of giving female children prosthetic penis packers, which can be purchased on the internet and at trans youth conferences for children as young as five years old. Adults haven’t actively and enthusiastically supported a child’s body dysmorphia in this way before. They also do not know if failing to provide any therapy to help said child accept the reality of her biology will lead to a medicalized path before full brain maturation.
The above quotes also do not address the reality that social transitions are going to lead to the early use of hormone blockers, which are now routine, for children as young as ten. Children on blockers rarely desist in studies that have tracked outcomes (see here and here). Whether or not this is because they would be trans-identitfied adults is unknown. It is not unreasonable to postulate the use of puberty blockers prevents desistance for children who would have outgrown GD in the past if they were allowed to pass through natal puberty. The scientific community has not demonstrated that lack of desistance is due to near-perfect screening techniques, nor have they explained why their cohorts, unlike all past cohorts, do not contain desisters.
In regards to the comment about youth having the option to choose not to have surgery, males put on hormone blockers early in puberty who go on to cross-sex hormones will face more difficulty if they desire “bottom surgery.” Male youth who have not completed natal puberty will require a colon graft, stomach lining graft, or skin graft to mimic any (female) adult appearing normalcy because hormone blockers to cross-sex hormones stunt sex organ growth in males. Again, this process can begin at 11 years old.
Evidence social transitions may in fact increase persistence
Below is another quote from Olson and Durwood:
Despite the recent alarmist calls about movements to persuade parents to socially transition their children to another gender and worry that doing so sets them up for a lifetime of hormone and surgical treatment, we know of no evidence suggesting that this is an issue.
This is an "argument from ignorance" that does nothing to prove early social transitions do not track children into medical transition by affecting their psychological development. There is also no reason why "we" would have any "evidence" of this, as they are implementing this new protocol with no control group. Kristina Olson is a scientist who graduated from Harvard and taught at Yale. She heads the Social Cognitive Development Lab at the University of Washington and has researched the effects of adult attitudes on children. In this article, she doesn't consider the impact on "social cognitive development" in borderline dysphoric youth who've made a full-time gender social transition.
It would be unusual for Olson and Durwood not to have seen some information regarding social transition and desistance in Steensma (2013). There is some evidence that social transitions may increase persistence. The data is limited and a small sample-size.
Dr. Ken Zucker, (due to issues around early childhood development, is concerned that early social transitions are going to solidify a trans identify (and thus a medicalized trajectory) in children who would otherwise outgrow gender dysphoria. This, explains why he helped some young people at his clinic transition, but only after very careful screening. Yet, being more careful may protect desisters but cause stress in persisters (a moral dilemma). Below are examples from his USPATH presentation (2017) from which he was eventually ejected due to trans activist complaints and successful attempts to shut down discussion of desistance research:
USPATH Presentation, 2017, Dr. Ken Zucker
Here, persistence correlates with a social transition. Indeed, the more dysphoric children were the ones most likely to transition socially. Still, researchers have no idea if this can also create false positives, as many desisters were DSM positive. The issue is that gender dysphoria really appears to be more a spectrum of severity than an either-or, and there is other evidence that supports other mental health issues and the environment affects gender dysphoria.
Anecdotally, the social transition-to-blocker protocol may increase persistence. More study is needed.
Not all gender professionals support an early social transition
Other gender professionals and scientists believe in a cautious approach rather than social affirmation.
Hill et al. [17] advocate an affirmative intervention, helping parents to support their child’s declared sex rather than attempting to have the child conform to their natal sex. There is an increasing parental support for young children living as their desired sex; however, desisters may struggle with returning to live as their natal sex when their original desire to live as the opposite sex had been so strongly supported and encouraged by parents and providers, and even accepted by peers.
Steensma expresses support for the “watchful waiting” or “Dutch model” approach:
We would counsel them ... that it's okay to express your feelings, your interests, to show your behaviors. But with certain steps like a name change, or a pronoun change, with a result that maybe others will only perceive you as a girl — that's somewhere where we say, ‘Okay, maybe you should explore things without taking steps that are hard to reverse.’
And:
If a child transitions, it is not just, ‘Oh, we do the transition and we go on with our life.’ It has a huge impact on the child, on the family and their environment.’
A paper authored by Steensma, “Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study”:
Given our findings that some girls, who were almost (but not even entirely) living as boys in their childhood years, experienced great trouble when they wanted to return to the female gender role, we believe that parents and caregivers should fully realize the unpredictability of their child’s psychosexual outcome…They may help their child to handle their gender variance in a supportive way, but without taking social steps long before puberty, which are hard to reverse.
The below quotes speak to the concerns of psychologists at the Tavistock clinic in England have:
Early social transition, they believe, can create a false impression: children start to believe growing up as the opposite gender will automatically follow putting on a dress and changing a name. “When, actually, we know it requires a lot of hard work and medical intervention to change the body,” says Dr Wren. “That’s not to be negative about it, because people go through it and have great lives. But the child might think, ‘Well, I’m growing up as a girl, aren’t I?” And you don’t want to shatter that and explain vaginoplasty to a six-year-old.”
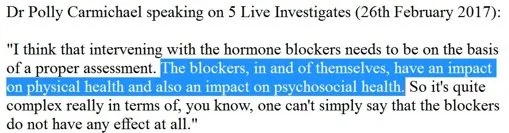
And also from a Tavistock psychologist Polly Carmichael, in The Guardian:
“If a lot has been invested in living in a gender role, then, potentially, it is difficult for young people to say: ‘Well, actually I don’t feel like that any more.’ Parents rightly want to support their child. Parents report that many young people who do make a social transition are much happier, that they’re functioning much better – which is why there isn’t a right and wrong. It’s about that child being able to carry on with general development, be in school. If transitioning facilitates that, then that’s positive, but how do we keep in mind a diversity of outcomes?” She pauses.
In Britain, the Royal College took down a link to an extremely pro early social and medical transition support group called Mermaids. They placed a comment expressing support for the watchful waiting approach and not the affirmative model:

Other skeptical scientists include Debra Soh, Michael Bailey, Eric Vilain, Susan Bradley, and the multiple mental health professionals from the GDworkinggroup.com.
Diane Ehrensaft believes the risk of social transitions are worth it (Ehrensaft 2018):
Many of the risks and benefits of social transition or the lack thereof have been alluded to in each of the previous sections, especially in the discussion about the controversies that are inherent in an approach that embodies both positive and potentially negative effects. What seems clear from the both the current research and clinical wisdom is that the benefits significantly outweigh the risks.
But Ehrensaft hasn’t employed any methods to determine if the benefits do outweigh the risks or if her protocol is over-medicalizing youth with GD (a major medical ethics problem). She instead employs a system of her observational diagnoses of “apples, oranges, and fruit salad” to categorize children. She has indicated she thinks worrying about over-medicalization is transphobic (see linked paper). Many people in the gay and lesbian community, as well as parents of gender-atypical youth, question the affirmation model because of concern that it may lead their possibly pre-same-sex attracted (or in some cases straight) minors down a path of sterilization and hormone prescription dependency. This outcome could constitute a human rights violation on par with allowing a trans child to mature before medically altering their body, putting them through a puberty they do not want. Without more evidence, these opinions about who is harmed more and how grievously could be considered subjective and tribally motivated. For an objective review of the costs/benefits of youth transitions see moral dilemmas.
Richard Green, one of the pioneers of transgender research, unlike Ehrensaft and the above-mentioned gender transition professionals, worries that:
An associated risk, as noted below, is the potential conflict associated with the decision to return to the natal sex. A long-term potential risk of transition could be promoting adult gender dysphoria requiring treatment with possibly problematic hormonal and surgical procedures that might have been avoided.
This quote about a psychiatrist in the United States where social transition is being pushed the hardest:
There are mental health professionals in the U.S. who agree (social transitions may be risky). Dr. Jack Drescher is a clinical professor of psychiatry at Columbia University; he served on the American Psychiatric Association's committee that revised the diagnosis of gender identity disorder in 2013. He said gender affirmative therapists have never proven they can successfully identify those kids who will stick with transgender identity.
He also says there’s no evidence to back a corollary belief, that kids who might later need to “detransition” back to their original gender will not suffer any long-lasting psychological effects.
“This is what they believe, but it's not based on research,” he said of gender affirmative clinicians. “This is a meme, not really a piece of scientific finding.”
Kristina Olson, Lily Durwood, Diane Ehrensaft, Dr. Forcier, Dr. Olson-Kennedy, as well as other mental and medical health entities and “LGBT” organizations, downplay or even dismiss the above concerns even though there is no actual research to prove that social transitions are “fully reversible” (while Steensma (2013) indicates they may not be). While not socially transitioning youth may have negative consequences on the child’s stress level, making it a non-neutral action, there is no evidence that intense validation and positive feedback are neutral actions. Considering a child will be living the majority of their formative years as the opposite sex, it is a valid concern that social transition will prevent desistance. The mental health and scientific communities need to discern what’s currently unknown about the effects of early social transitions before it is possible to ethically claim they are “fully reversible.” We look to our scientists to offer truth.
D. Unsubstantiated claims it is known that hormone blockers are fully reversible & that they are beneficial to the child’s decision-making process about their gender
Puberty does resume if hormone blockers given to an adolescent are stopped, but it takes 6-18 months to resume normally. This is a long time for a tween or teen through a period of crucial brain development and organization. This doesn’t mean there are no long-term health or cognitive consequences from taking Lupron or other hormone blockers, and this does not mean hormone blockers do not affect the youth’s gender identity formation. Therapists, doctors, activists, “LGBT” organizations, and journalists can not know if all of the effects of hormone blockers are “fully reversible” without more research and a control group to test for the psychological effects. Many would consider control groups, in this case, to be unethical.
Even if the effects are reversible, hormone blockers create another problem, according to this concerned parent:
…it freezes youngsters in a prolonged childhood, secluding them from certain aspects of reality and isolating them from peer groups.
And it may also have a negative impact on the youth’s sexual exploration and sexual identity development:
We know very little about the capacity for sexual pleasure in a natal male who proceeds to genital reconstruction after puberty blockade. But we know for certain that blockers reduce libido: they are after all also used to chemically castrate sex offenders. The medical treatment for sex offenders available on the NHS includes GnRH agonists used as ‘antilibidinal medication’. ‘Antilibidinal medication is associated with a range of side effects’ the guidance for clinicians warns, ‘including the risk of liver damage, breast growth, hot flushes, depression and a decrease in bone density.’ Puberty blockers put a natal female into a ‘pseudomenopause’.
Physical effects of giving children hormone blockers to cross-sex hormones may not be reversible.
Several women who received Lupron to prevent precocious puberty are claiming side effects from using this drug, some of them are serious, and the FDA has recently updated some warnings about Lupron:
More than 10,000 adverse event reports complaining about the side effects of a commonly used drug called Lupron have been filed with the Food and Drug Administration, according to a recent report by Kaiser Health News, yet both the drug-maker and the FDA have so far failed to warn pediatric patients or their parents about the drug’s side effects.
The New Atlantis is a conservative journal but the argument these doctors are presenting is reasonable here:
Because the major studies of puberty suppression have not reported results of patients who have withdrawn from treatment and then resumed the puberty typical of their sex, we also do not know how normally the primary and secondary sex characteristics will develop in adolescents whose puberty has been artificially suppressed beginning at age 12. And so the claim that puberty suppression for adolescents with gender dysphoria is “reversible” is based on speculation, not rigorous analysis of scientific data.
Some studies indicate possible problems with bone loss and loss of IQ points with hormone blocker use in children. Also, aside from possible negative physical consequences of Lupron use long-term, the physical effects of giving children hormone blockers to cross-sex hormones are not reversible. This process sterilizes males and females and, in males, stunts genital growth (micro penis”) and can cause sexual dysfunction. For a more comprehensive discussion of the physical effects of giving children puberty blockers, see here.
General risks of Lupron used to treat various conditions are discussed In “Lupron: Déjà Vu All Over Again”:
Alice Dreger raises concerns about a pervasive pattern of non-evidence based assumptions driving practices in pediatric endocrinology…
What’s particularly disturbing, then, given that Lupron is believed to carry significant risks, is how badly pediatric endocrinology has tracked its usage of this drug. Many—very possibly most—pediatric uses of it have occurred via academic medical centers, yet we have surprisingly little solid prospective data on the long-term benefits and harms.
You’d think that the pediatric specialty that may have given cancer to women treated with estrogen because as girls they were ‘at risk’ of growing up tall might be pretty careful with other drugs. You’d think that it would be especially cautious about treating kids with hormone blockers because they are ‘at risk’ of growing up short.
Pediatric endocrinology, I’m talking to you.
Multiple statements on the “reversibility” of hormone blockers
Despite these reports of problems with Lupron and the reality that no one knows the psychological effects of hormone blockers on gender identity because no one has done a study with a control group, many people and entities in mental health and medicine claim blockers are “fully reversible.” Doctors in The New Atlantis point out what they believe are the ethical problems with these positive statements about Lupron (or other blockers) and document just a few examples of the assertion that hormone blockers are fully reversible:
‘Claims of “Reversibility’
● The Dutch scientists who developed the protocol for puberty suppression describe it as “fully reversible.”[103]
● Pediatric endocrinologist Daniel Metzger says that “the effect of the puberty-blocking drugs is reversible.”[104]
● Norman Spack, a physician at Boston’s Children Hospital who treats gender dysphoria, describes puberty-suppressing drugs as “totally reversible.”[105]
● In a review of the research on puberty-blocking drugs for an LGBT advocacy group, Laura E. Kuper, a researcher focused on transgender health, describes puberty blocking as “fully reversible.”[106]
● Transgender journalist Mitch Kellaway, writing for the website Advocate.com about how “blocking puberty is beneficial for transgender youth,” describes puberty blocking as “fully reversible.”[107]
● In another Advocate.com story about puberty blocking, transgender activist Andrea James writes that “the treatment is reversible.”[108]
● Bioethicist Arthur Caplan has described puberty blocking as reversible, saying that “if it’s decided to stop the treatment, puberty will resume.”[109]
● Pediatric endocrinologists Christopher P. Houk and Peter A. Lee write that puberty suppression in children with gender dysphoria is “reversible.”[110]
The article also notes that the HRC, one of the largest “LGBT” rights organizations in the U.S., claims that blockers are reversible.
The following are a few more examples of doctors and mental health professionals claiming they know blockers are “fully reversible”:
WPATH describes blockers as “fully reversible”
Hembree et al“ (i) their use gives adolescents more time to explore their gender nonconformity and other developmental issues;”
Dr. Johanna Olson states, “So, what a lot of people want to understand is, ‘If I give my child this blocker, can I take it away, if at the end of a certain amount of time they no longer have a trans-gender identity, or they don’t want to continue on to pursue a transition with cross-sex hormones.’ The answer to that is, ‘Yes.’ They are reversible. You can take them off without any problems or major medical problems.’”
UCSF Benioff Children's Hospital, “These hormones can safely suppress puberty by blocking the production of the principal sex hormones: estrogen and testosterone. Fully reversible…
Dr. Michelle Forcier, “The risk of not giving puberty blockers and the harm for continued development in the “wrong” gender far outweighs the minimal risks of totally reversible blockers.”
American College of Osteopathic Pediatricians, “to prevent the consequences of going through a puberty that doesn’t match a transgender child’s identity, healthcare providers may use fully reversible medications that put puberty on hold.”
Therapists, doctors, “LGBT” organizations, and journalists also advertise the benefit of blockers in helping the youth to make better decisions. Without a control group to assess the effect of blockers on desistance (almost no minors desist on blockers), these entities and individuals are making this claim without having evidence to support this assertion. The “buying time” argument doesn’t take into consideration that blockers may be preventing the very hormones and processes that help the youth align with their natal sex. Blockers alleviate stress in some youth. However, stress around gender may be part of the process of learning to accept it.
Dr. Annelou de Vries, “Since puberty suppression is a fully reversible medical intervention, it provides adolescents and their families with time to explore their gender dysphoric feelings, and [to] make a more definite decision regarding the first steps of actual gender reassignment treatment at a later age.
The Dutch scientists state puberty suppression, “give adolescents, together with the attending health professional, more time to explore their gender identity, without the distress of the developing secondary sex characteristics. The precision of the diagnosis may thus be improved.”
American College of Osteopathic Pediatricians, “Delaying puberty gives the child time “to explore gender-related feelings and options.”
WPATH says, “Their use gives adolescents more time to explore their gender nonconformity and other developmental issues”
Gender dysphoria expert Professor Ashley Grossman, “insists this puberty blocking treatment ‘does not harm children’ but gives them extra time to make the crucial decision.”
Dr. Rob Garofalo, “That’s really what these pubertal blockers do…They allow these families the opportunity to hit a pause button, to prevent natal puberty … until we know that that’s either the right or the wrong direction for their particular child.”
Dr. Steve Rosenthal, “It gives them more time to understand who they are without the clock ticking,” and“ GNRH agents have been used for many years and have been found to be very effective and specific for blocking puberty in a completely reversible manner.”
Michelle Forcier, “And so we use the puberty blocker which are totally reversible, nothing for the future changes. It can all go back to the way it’s supposed to be biologically.” (6:33-6:48)
UCSF Benioff Children's Hospital, “Fully reversible, this treatment gives young people time to achieve greater self-awareness of their gender identification. If and when appropriate, our experts may administer cross-gender sex hormones.”
Professor Ashley Grossman, “There is a bit of a call from the public that they are being over-diagnosed and people get disturbed about medicating children but with puberty blockers they are not being treated, just given time.”
Polly Charmichael, “The good thing about [puberty blockers] is if you stop the injections it is like pressing a start button, and the body just carries on developing as it would if you hadn’t taken the injections.” She has made more nuanced comments as well (see below).
Hormone blockers may effect youth gender identity & increase persistence
No doctor or mental healthcare professional knows for sure what the influences of hormone blockers will be on the gender development of young people, especially when giving blockers to children as young as 9 (females) or 11 (males) doesn’t give youth any meaningful amount of time spent in puberty. Clinicians cannot know the full effects of early puberty suppression without performing a study with a control group with a cohort who goes into puberty without blockers (there are issues with control groups & human subjects). The extremely low desistance rate of children put on hormone blockers should lead to serious questions. In addition, affirmative model advocates do not hold a consensus opinion on blocker reversibility. Many gender professionals themselves worry that they are solidifying gender nonconforming children, disproportionately likely to be gay, lesbian, bisexual, or autism spectrum, into a medical transition pathway.
Polly Carmichael is the director of GIDS (Gender Identity Services) and a consultant clinical psychologist at Tavistock, a gender clinic for youth in Britain. Here she is quoted in The Guardian:
Carmichael says it’s very important for young people to experience some of their own puberty. ‘The blocker is said to be completely reversible, which is disingenuous because nothing’s completely reversible. It might be that the introduction of natal hormones [those you are born with] at puberty has an impact on the trajectory of gender dysphoria.’ Even though the idea of experiencing any “natural” puberty might horrify the Kings and the Wilsons, by inhibiting it completely, Tom and Julia might be denied the chance to explore fully who they are.
The below screen shot is from a live radio event:
Dr. Wren from the same clinic expresses a similar viewpoint:
The younger ones can really, really want to be girls or boys, and then they can give that up and their relationship to their bodies can settle down quite comfortably. If we can help some of those young people through adolescence, they might make a different choice later.
The New Atlantis is a conservative journal and not friendly to issues such as same-sex marriage but they still make valid arguments in the quotes below:
One common argument based on the idea that puberty suppression is a reversible and prudent first step is that it can, as the Dutch scientists put it, “give adolescents, together with the attending health professional, more time to explore their gender identity, without the distress of the developing secondary sex characteristics. The precision of the diagnosis may thus be improved.”[114] There is much that is strange about this argument. It presumes that natural sex characteristics interfere with the “exploration” of gender identity, when one would expect that the development of natural sex characteristics might contribute to the natural consolidation of one’s gender identity. It also presumes that interfering with the development of natural sex characteristics can allow for a more accurate diagnosis of the gender identity of the child. But it seems equally plausible that the interference with normal pubertal development will influence the gender identity of the child by reducing the prospects for developing a gender identity corresponding to his or her biological sex.
And here is a quote from “Early Medical Treatment of Children and Adolescents With Gender Dysphoria: An Empirical Ethical Study”:
In the literature, the concern is raised that interrupting the development of secondary sex characteristics may disrupt the development of a gender identity during puberty that is congruent with the assigned gender. The interviews and questionnaires show that some treatment teams share this view.
In the quote below a gender dysphoria professional is skeptical about the safety of Lupron and the lax transition process in Britain (which has a stricter process than many places in the United States):
She is scathing, too, about puberty-blocking drugs such as Lupron – prescribed off-label, without any long-term studies upon the developing body and brain – which “pause” development, theoretically to give a child a year for reflection. In practice, almost 100 per cent of children on blockers proceed to cross-gender hormones.(This causes certain sterility: the gametes never mature enough for eggs or sperm to be banked.) “That year on blockers should be when we have deep, intensive regular therapy. We should ask, ‘What is a girl? What is a boy?’ Instead we barely see them, their peers go through puberty and leave them behind, which makes them even more anxious and desperate to transition.”
This German study raises several points about how blockers prevent some critical life experiences that come from natural puberty:
A treatment of this kind changes the individual's sexual experience both in fantasy and in behavior. It restricts sexual appetite and functionality and thereby prevents the individual from having age-appropriate (socio-)sexual experiences that he or she can then evaluate in the framework of the diagnostic-therapeutic process. As a result, it becomes nearly impossible to discover the sexual preference structure and ultimate gender identity developing under the influence of the native sex hormones
And:
It is not known with any certainty at present how hormone therapy before the end of puberty might affect the further development of gender identity, or to what extent it might even iatrogenically induce persistence of GID. Thus, even in a case of treatment retrospectively judged to have been successful, one cannot necessarily assume that the patient's transsexualism was a predetermined matter at the outset. Children and adolescents generally lack the emotional and cognitive maturity needed to consent.
E. Obscuring desistance
Understandably, trans activists want to downplay desistance research data around children with gender dysphoria because it creates roadblocks to trans youth socially and medically transitioning. They want social support and medical inventions to improve long-term mental health and passing ability as early as possible. There are, however, doctors and therapists, entities who the public turns to for non-biased information, who make statements that appear to downplay desistance without providing conclusive evidence it doesn’t exist in truly dysphoric youth. Some may even indicate they are invested in the “desistance is a myth” narrative but cannot offer scientifically valid proof their protocols aren’t increasing persistence. Affirmative model advocates also constantly emphasize methodological imperfections (something most trans research has) in studies that show desistance. Currently, there is no proof that a “true trans child” can always be differentiated from a GNC likely pre-gay/lesbian child.
For a look at desistance research see Topic 1.
Multiple statements by affirmative model mental & medical health professionals seeming to downplay desistance
Michelle Forcier (2:50) said in an interview to NBC that, “Kid’s rarely change their minds about their gender identity.”
1) While studies and diagnosis are imperfect, the number of children who had an official DSM diagnosis of gender dysphoria (pre-DSM-V) from Dr. Zucker’s review (USPATH, 2017) is taken from these studies:
The results of children with diagnosable gender dysphoria who desisted were averaged to be 67%. While perhaps not all 67% would have been diagnosed under DSM-V (with somewhat stricter criteria), it is unlikely none would have been diagnosed under the current guidelines.
2) Forcier made this claim on a national network, which helped spread the mistaken belief children don’t desist. Forcier’s claim is often repeated in trans child support groups where parents are turning to for information on how to support their children best.
3) If Forcier rarely sees desistance in the pro-transition environment she works in, it’s reasonable to posit that affirmation increases persistence rates. Remember, other clinicians such as Steensma and Carmichael say they observe desistance.
Norman Spack says this in a quote from a quote in The Guardian:
The NHS guidelines currently state that no children be given this hormone treatment until they are around 16. Spack sees the age as arbitrary, and often cruel. ‘Why wait?’ he asks.
Reasons it may be beneficial to wait:
1) Desistance rates from all studies in the past necessitate more certainty that doctors aren’t irrevocably, permanently, medically altering the bodies of minors that are healthy, functioning, and intact.
2) Comments from other gender clinicians stating sometimes youth need to experience some actual time in puberty to desist.
3) Early blockers to cross-sex hormones stunt sexual maturation in males, making the preferred method for vaginoplasty impossible and possibly eradicating future adult sexual function.
4) Early transitions sterilize these youths
5) Early transition carries unknown cancer and cardiac risks, and hormone blocker side effects may be serious.
Waiting may not be a neutral option due to distress and unwanted secondary sex characteristics. But these reasons also seem like legitimate subjects to discuss when talking to the public.
Norman Spack also talks about how adolescence is a time when trans children remain dysphoric:
Thankfully there’s something that defines who’s the real deal—and that’s their attitude toward puberty. Even the sternest critics will say that, in their experience, when children don’t accept their birthright to the puberty that’s consistent with their sex, then those children are almost certain to be transgender. We can bank on that, but we need to confirm it with the extensive psychological testing that we do.
Unfortunately, this is not always true, and the rapidly changing demographics of adolescent gender dysphoria show large numbers of females (often same-sex attracted, autism spectrum, or with past trauma) who never experienced any child dysphoria at all. Yet, therapists and doctors in the West will transition teenagers even when they didn’t have childhood gender dysphoria. There are many examples provided on this website of teenagers, particularly female ones, who identified as trans for several years and then desisted. It is an undeniable fact that teenagers who would be diagnosed under DSM-V criteria have desisted.
While adolescent persistence may be a good indication the youth will always be trans if they have had gender dysphoria from early childhood, it is not a sure way to diagnose some of these later onset cases.
Dianne Ehrensaft states in (Ehrensaft 2018):
The conservative watchful waiting approach to the treatment of gender-expansive children that is in the current WPATH SOC appears to be based on binary notions of gender and pathologizing views of gender diversity.
Is this possibly a dismissive characterization and demonization of concern?
1) Many people concerned about medicalizing minors are social and political liberals who fully support gender nonconforming behavior and are often LGB themselves. The concern here is that the child, based on decisions made as a minor, will be over-medicalized and experience a lifetime of consequences.
2) Ethical guidelines for mental health and medical professionals recommend less drastic treatments before more drastic treatment is applied. Watchful waiting is mindful of this and aligns with every other medical treatment approach to a condition.
3) Some of the parents most vocal and enthusiastic about transitioning their children have been openly homophobic right-wing Christians who said they worried their children were gay and were happy to reinforce their children as “binary.” Ehrensaft doesn’t address the role familial and societal homophobia could play in this matter (see here and here and here). Enthusiasm to affirm a child as trans may not always be the most progressive response and may be a regressive, bigoted one.
Madeline Deutsch, clinical director at the University of California San Francisco’s Center of Excellence for Transgender Health, is quoted in this ThinkProgress piece, which contains some comments that are factually questionable about desistance research:
Likewise, Deutsch finds it conspicuous how few transgender researchers were actually involved in the desistance studies. Skepticism about letting kids transition, she said, “is driven underlying by a field of predominantly non-transgender researchers who are trying to turn this into some kind of field that is of interest and that is curious so they can generate more research and publications. It is not something that is being driven by the community…It’s not that she thinks only trans people should do this kind of research, but she questions the motives of people who aren’t working with the trans community to study the trans community.
1) Deutsch's statements are relatively common among pro-early transition doctors and therapists. It may be reasonable to make the point that desistance rates in the past were likely inflated due to including gender-nonconforming youth who were sub-threshold dysphoric in desistance statistics. However, Deutsch and Keo-Meier's comments seem to deny the existence of desistance altogether, even though other gender clinicians have clearly stated the "no youth desist" claim defies their clinical experiences. Here is a review of more recent studies with desistance data summarized by renowned sexologist James Cantor. Even if the diagnostics weren't perfect, the number of desisters is still very high and warrants concern.
2) In regards to Deutsch's comment about researchers weighing in who aren't trans, trans-identified people's perspectives are essential in the treatment of dysphoric people. However, it is not appropriate for social and medical science to be agenda and activist-driven. The purpose of social science and medicine is to provide evidence-based care that treats trans patients and makes sure children, teens, and young adults are not unnecessarily medically disfigured. Trans activism is doing severe damage to honest scientific debates about the long-term safety of medical transition.
3) It is equally rational to "question the motives" of researchers like Deutsch who work with the trans community, and it is valid to ask whether or not a confirmation bias is driving them to hide the risks of socially and medically transitioning minors who are GNC, LGB, autistic, or just generally confused. There is a long history of confirmation bias found among scientists, and bias comes from all directions. It may be challenging for a gender-affirming therapist to admit the protocol they advocate for will lead to the unnecessary castration of effeminate gay boys at an age where consent is legally debatable.
Kids do roll through a lot of things as they go through identity formation but our gender is a core part of who we are and we actually all know what our gender is and have pretty solid gender identity by the age of 3 or 4 years old.
This statement may be true for most people.
However:
1) Gender dysphoric children do desist.
2) Detransition and regret are real, and the numbers appear to be increasing (see here)
3) There are many anecdotal accounts of gays and lesbians, in particular, who said they outgrew GD.
4) There is a section below on who Diane Ehrensaft calls “fruit salads.” Gender affirming therapists almost all acknowledge gender is solid in some people but fluid in others. They emphasize support of social and medical transition. They do not consider the risk this poses to the “fruit salads” who may make the wrong medical decisions as children, teens, or young adults.
Olson-Kennedy responding to an individual who asked about desistance and regret (USPATH, 2017):
Not everybody tells us about their gender in childhood. In fact, most people don’t. And this is really critical…I’ve had a lot of people come into my office with adolescents. But my kid was saying I am a girl, I am a boy or I am neither. Or something else entirely when they were three. So, they are not trans, they don’t meet the check list. It’s really important to understand that it’s not that someone is more trans than another person. The way it rolls. The way gender rolls. So, I think this is really important that as providers we need to give this message…It’s extraordinarily rare that someone comes out in early childhood…That being said it makes sense that trans adults started off as trans kids (audience laughs)…But I will tell you what I hear which is the narrative that someone isn’t trans enough. That’s nonsense. We gotta stop that narrative.
1) This comment rings true for the children who will grow up to be trans adults, seeing denying them transition as unethical. Transgender people view it as patronizing and paternalistic to prevent transition for children and adults who feel they know who they are and what they want. But medical providers are obligated to protect all youth, including those who will become desisters.
2) In regards to Olson-Kennedy’s argument that no one should worry about a child identifying as trans temporarily and desisting or not being “trans enough” for medical care: just because it is true that all trans adults were trans children or trans teens, that is not proof that all gender dysphoric minors are trans.
Olson-Kennedy again (Gender Odyssey, 2017):
Identity formation is the major task of adolescence and the urge for what is true about the self is the driving force behind many commitments behind identity. Gender is not part of that. I really want to be clear about this. We are born with our gender. When we come to know if it’s different than our assigned sex at birth is variable depending on persons to person. But it’s not a thing!..that teenagers go, “I might be a different gender.” That’s not a thing. That’s not a thing that all adolescents experience.
1) Not all adolescents question their gender, but trans identification is transient in children and, increasingly, in adolescent populations. Quite a few examples of youth who desisted (here and here) can be found on 4thwavenow, a website run by parents skeptical of medically transitioning minors. These young people all had transient transgender identities for as long as several years. For them, gender dysphoria was not a brief phase. Olson-Kennedy is aware of this website and references it in the same seminar. These youths not only had temporary trans identities but said cultural factors and their struggles with identity formation as it relates to adolescence itself contributed to their temporary trans identification.
Dr. Joshua Safer is the director of the Endocrinology Fellowship Training Program at Boston Medical center and an associate professor at Boston University School of Medicine whose research focuses on the biological underpinnings of gender identity. While he’s heard the arguments suggesting that a shift in gender balance at clinics serving trans youth means that children are being pushed into being trans, he’s emphatic that there’s no evidence to support the idea that a person’s gender identity can be changed.
“I know that parents out there think ‘If I let my kid experiment then somehow my kid will brainwash himself or herself to go down this challenging path,’ ” he said. “But if your kid’s not trans, they won’t end up identifying as trans. One of the big things I push is that the evidence is for gender identity being biological—as scientists we should be thinking about it as, okay, the biology is what it is, and so then what’s the treatment approach?”
Dr. Safer also advocates for lowering the age of consent:
We recognized that there’s no biological logic to a cutoff of 16,” explained Joshua Safer, an endocrinologist at Boston University School of Medicine who was also instrumental in revising the guidelines. “There are kids with a clear gender identity out there and there is no reason to make them wait for some legal line when we can already be helping them with their biological reality.
1) The biological essentialist argument may be true for many or even most trans people. However, there is much evidence of cultural factors, other mental health factors, internalized and externalized homophobia, and parental factors influencing trans identification. Hard biological determinism is not the only cause of all decisions to medically transition. More on the “nature versus nurture” conversation can be found here.
2) In one of the most recent surveys of trans-identified youth, there were over nine times more trans boys (biological females) than trans girls and many more non-binary-identified youth who are primarily female. It would be interesting to hear Joshua Safer explain why, until recently, there were never more trans biological female teenagers than male ones:

For more on the increasing numbers of trans-identified females, see here.
3) Dr. Safer’s pro-medical transition position is not surprising because he is supportive of the off-label use of a drug for horses that comes with warnings from the FDA for MtFs to induce lactation so that MtFs can breastfeed newborn babies:
Dr. Joshua D. Safer, medical director of transgender medicine and surgery at Boston Medical Center, called the study “a very big deal” and said he expected it to become very popular among transgender women.
Methodological flaws arguments don’t prove desistance numbers are statistically irrelevant
In a sincere desire to support dysphoric children, there is a concerted effort to get the public on board with the enthusiastic social transition of children. Part of this seems to be through efforts to downplay previous studies with high desistance rates. These studies hinder embracing the social and medical transition of youth, which may be why affirmative model advocates focus heavily on the imperfections of the studies. First, several of these studies have desistance / persistence data on DSM-positive youth, even if the criteria are imperfect. In addition, most studies have methodological flaws (including studies affirmative model advocates approve of). And finally, even if desistance rates were inflated in some older studies because GNC and not seriously dysphoric youth were taken to gender clinics, inflation does not mean statistically insignificant numbers.
The watchful waiting approach evolved from the first model of care for transgender children developed in the Netherlands, often called the Dutch Protocol. The Dutch Protocol is informed by the belief that gender dysphoria, or a transgender identity, persists into adolescence in only a small minority of people (Steensma & Cohen-Kettenis, 2011). As outlined earlier, this research suffers from potential methodological flaws and the way the data have been interpreted suggests that providers be more concerned about the rare cisgender child being treated for gender dysphoria at the expense of the many transgender and gender-expansive children who would be helped if social transition were an option. The result of this interpretation has the potential to have profound negative impacts on treatment practices in pediatric transgender healthcare (Winters, 2014)…
Lastly, the research results may include inflated percentages of desisters, as counted among their number were those who did not return to the clinic for care; therefore, reporting all patients lost to attrition as “desisters” rep- resents an assumption that has never been validated, and rates of persisters and desisters cannot be verified unless these patients are tracked down…
And:
Desistance rates cannot be accurately determined without valid measures of gender identity in children. Yet, at the time the research was conducted, no valid measures of gender identity were available aside from child statements which could be influenced by any number of factors, and which conflated statements about gen- der-related wishes with statements about actual identity. In other words, if cisgender children were incorrectly thought to be transgender in early research, rates of desistence would be inflated. This is an important issue, as it is possible that gender identity is as stable in gender-expansive children as cisgender children.
1) Ehrensaft claims that the "rare" "cisgender" dysphoric child who would outgrow gender dysphoria but doctors instead may medically deface is not a reason to withhold "care" for persisters. One could make an argument for this viewpoint. But as of spring 2019, we are unaware of any research from UCSF, where Ehrensaft treats youth, proving her claim that these children are rare. Other clinicians believe desistance is quite common, but that early transition may prevent it from happening.
2) Ehrensaft states, "Desistance rates cannot be accurately determined without valid measures of gender identity in children." Yet, as of spring 2019, we are unaware of any research coming out of UCSF that presents diagnostics for an accurate screening process for "true trans children." One measure she, as well as Kristina Olson, uses is the idea that children who say they are trans (and are not just wishing to be the opposite sex) are "trans" (see below). Some examples of Ehrensaft's diagnostic approach are here. Still, much of it indicates many gray area children, the ones people fear may be at serious risk for being over-medicalized before reaching full brain maturation.
Here is a breakdown and criticism of typical arguments used to downplay desistance studies (too many lost-to follow-ups, too many GNC/not GD kids counted.
One example, of the “lost to follow ups may still be trans” argument:
Reference 47 was a one-and-a-half page commentary which off-handedly mentions criticisms previously made of three of the eleven outcome studies of GD children, but does not provide any analysis or discussion (Olson, 2016). The only specific claim was that studies (whether early or late) had limited follow-up periods—the logic being that had outcome researchers lengthened the follow-up period, then people who seemed to have desisted might have returned to the clinic as cases of “persistence-after-interruption.” Although one could debate the merits of that prediction, AAP (and Olson) instead simply withheld from the reader the result from testing that prediction directly: Steensma and Cohen-Kettenis (2015) conducted another analysis of their cohort, by then ages 19–28 (mean age 25.9 years), and found that 3.3% (5 people of the sample of 150) later returned. That is, the childhood sample showing 70.0% desistence instead showed 66.7% desistance in long-term follow-up. It is up to the reader to decide whether that difference challenges the aforementioned conclusion that that majority of GD children cease to want to transition by puberty or represents a grasping at straws.
Michele Angelo and Alisa Bowmen both make this same argument about Steensma’s data but it is not accurate:
[Michele] Angello and [Alisa] Bowman explain why this assumption is so misguided: They might have switched doctors, moved, or worse, committed suicide. Also, it’s common for transgender people to express their true gender, face an abundance of ridicule and harassment, and then repress it.
It’s the equivalent of a dentist who assumes that if patients stop coming back, that means that they’re no longer getting cavities.
Journalist Jesse Singal addresses this:
The problem is, Angello, Bowman, Keo-Meier, Ford, and, unfortunately, myself… we’re all wrong. Completely wrong. Steensma and his colleagues never simply assumed those 80 kids had desisted — they got in touch with most of them, and, true to that ‘assumption,’ they weren’t dysphoric.
Now, we could be forgiven for thinking they simply assumed those 80 kids were desisters — that paragraph above really is written in a confusing way. But if you read the study closely — always read the study closely! — it’s clear this isn’t what happened. Here’s what’s in the very next paragraph: “All 47 persisters participated in the study. Of the 80 desisters, 46 adolescents sent back the questioners (57.5%) and 6 (7.5%) adolescents refused to participate, but allowed their parents to fill out the parent questionnaires. Twenty-eight adolescents were classified as nonresponders: 12 (15%) did not send back the questionnaires despite follow-up contacts, another 12 (15.0%) were untraceable. In 4 cases (5.0%), the adolescents and the parents indicated that the GD from the past remitted, but these individuals refused to participate…
Now, it’s important to note that this group was less dysphoric at intake. Of the total 80 kids in the sample who stopped coming, 39.3% of boys and 58.3% of girls met the criteria for what used to be called Gender Identity Disorder, or GID.
So here is evidence that of 80 gender non conforming children who were brought to the clinic but were not dysphoric or did not return to the clinic but could not be reached (likely desisters) 39.3% and 58.3% had had GID. A smaller percent than the persisters but still significant.
In response to Temple et al 2018 making efforts to discount desistance stats due to methodological imperfections, Steensma explains how their 2013 study dealt with follow-ups:
We agree that the current persistence rates may go up if a different methodology would be used (see above), but the suggested reasons why non-responders may actually be persisters are unlikely and farfetched. For instance, the authors suggested that children were lost at follow-up because they moved out of the country, were being treated elsewhere in the Netherlands, or institutionalized. The chance that one of these situations occurred is, however, very low.
Colt Keo-Meier, a clinical child psychologist based in Houston, makes some statements seeming to support the “desistance is a myth” narrative, in a ThinkProgress piece. She asserts older studies just marked gender nonconforming (GNC) children as desisters:
When they were older, of course they didn’t transition because they weren’t transgender to start with.
Kristina Olson and Lily Durwood from the Trans Youth Project are quoted below from a piece who’s intention appears to be to assuage public fear early social transitions may harm borderline GNC youth. They admit desistance happens:
This is not to say that a transgender identity in childhood never desists in adulthood. The truth is that we do not know precisely how many transgender children will grow up to be transgender adults, because no long-term studies have recruited a large number of children who believe that they are members of the opposite sex nor separated the few they have included in past studies from the broader group of gender nonconforming children. Until the start of our project in 2013, we knew of no studies tracking large numbers of children who specifically identified as transgender in early childhood. Thus, while most popular articles on this topic imply that 80 percent of children with transgender identities will not grow up to be transgender adults, we believe it is more accurate to say that we have no good estimate. What little data do exist suggest that many transgender-identified young children do in fact become transgender-identified teens and adults.
In reality, as with almost all studies on the trans population, their own study is “methodologically flawed” in that they follow fully affirmed, socially transitioned children with no control group of parents who love and support their child, but promote a body acceptance model with transition as last resorts.
Another article ask questions of Robert Garofalo’s assertions about desistance:
Garofalo fails to mention the issues with using GnRH agonists in children. The article then goes on to say that “The handful of studies that do exist suggest that gender dysphoria persists in a minority of children, but they involved very few children and were done mostly abroad” which is incorrect. The article then goes on to acknowledge that the use of puberty-blockers is off-label, and even concedes that such uses of the drug, considering the length of time it is used for, and the effects of stalling puberty, are totally unresearched. Another pediatrician at Lurie, Lisa Simons, admits this:
Johanna Olson-Kennedy (Gender Odyssey, 2017) appears to downplay desistance in a Q&A for professionals.
But unfortunately...it’s important to recognize in that data, all of the people that were studied were prepubertal. They were children…We were only talking about, pretty much, children, boys who wanted to look like girls or act like girls, play with girl’s things, or wear clothes that girls would wear, blah blah blah.
For the most recent studies the criteria is not that different. They were under DSM-IV or III. DSM-V is somewhat more stringent. There are more similarities than differences between them.
Framing discussions of desistance as transphobic possibly to avoid ethics discussion around risks to desisting children
Some discussions of gender dysphoric children in affirming environments do not include questioning parental, peer, and other cultural effects on socially transitioned youth and their gender identity. Why is this?
Diane Ehrensaft offers a possible reason for this lack of discussion of the many cultural and environmental factors (see here) that influence gender dysphoria in at least some cases. It's considered transphobic to worry about it (Ehrensaft 2018). If worrying about borderline children is framed as transphobic, the concern is a culture where people are shamed for talking about desistance and are even afraid to bring it up. There is indeed discouragement of desistance discussions both at some gender conferences and in some trans support groups for parents.
Ehrensaft, in regards to desistance being a preferable outcome:
Furthermore, this is a value-laden statement suggesting that it is preferable for a child to avoid embracing a transgender or gender-expansive identity, and that diversity with regard to gender is inherently wrong and not as good as a cisgender identity. It also suggests that quality of life in childhood is negligible and can be sacrificed in the service of getting gender “right.”
Given that many people skeptical of the safety of transitioning children are socially and politically liberal, and many are LGB or trans themselves, the accusation of transphobia is more propaganda than truth in many cases. What is "value-laden" is that doctors should not medically alter a young, healthy body and endocrine system in ways that include castration and sterility before brain development and maturation is complete.
In “The myth of persistence: Response to “A critical commentary on follow-up studies and ‘desistance’ theories about transgender and gender non-conforming children,” Dr. Ken Zucker criticizes a pro-affirmative model study (which had many methodological flaws) and talks about how erasing the term “desistance” is a deliberate attempt at censorship:
At the end of their long ethical discourse about harm, Temple Newhook et al. (2018) conclude that “...longitudinal studies about identity ‘desistance’ or ‘persistence’ are not the best tools for understanding the needs of gender-nonconforming children.” Although I agree it should not be the only metric for understanding the needs of children with a diagnosis of gender dysphoria, the implicit message is something like this: Research on persistence and desistance should be suppressed: it should just disappear without a trace. This is empirical and intellectual “no platforming” at its worst. I find this ominous, but not surprising.
More from Dianne Ehrensaft:
Another concern that has been raised is that if a gender-expansive child is allowed to socially transition, then go on a GnRH agonist at Tanner Stage 2 of puberty, thereby never experiencing the puberty associated with their assigned sex, they will never have a full understanding and self-knowledge of their gender because they were denied the opportunity to experience the “correct” puberty. As stated previously, even if they appear happy and well-adjusted, from this transphobic perspective, being a transgender person is considered a poor outcome because of the discrimination they will face and the lifelong course of medical treatments they may require.
The approach towards all other physical and mental health conditions is that doctors employ the least extreme and invasive techniques first, graduating to more drastic measures. Doctors are morally obligated not to over-treat a patient with medicines and surgeries:
The conservative watchful waiting approach to the treatment of gender-expansive children that is in the current WPATH SOC appears to be based on binary notions of gender and pathologizing views of gender diversity. The studies used to support this stance conflate gender role and gender identity, which leads to a problematic interpretation of the results (Steensma et al., 2011).
Professionals who call for greater caution are not pathologizing trans children. The medical consequences can be dire (sterility, bone health, and possible effects on sexual function and cognition). There may be benefits for youth who persist and ultimately medically transition, such as intact fertility and intact genitals afforded by postponing transition.
Johanna Olson-Kennedy (WPATH Facebook June 8):
Only numbers out about the answer to this question about those who come out in adolescence are from the Dutch – 100% of their cohort had a trans identity at follow up. “Persistence” and “desistance” are another irrelevant binary that do not accurately represent the gender experiences of most trans people. Sadly, I think we are still asking questions that are rooted in easing the discomfort of cisgender people, whether that be parents, or providers. This need for a litmus testing of a “gold star trans person” is derailing to the mission of providing timely, thorough and appropriate patient centered care for trans individuals.
1) This quote demonstrates that some clinicians frame worrying about over-medicalizing minors as inherently transphobic and “cis normative.”
2) They attributed to “cis normative” people. But it is primarily LGB people who are very gender nonconforming as children and are most concerned about medicalization.
Olson-Kennedy (Gender Odyssey, 2017):
…the language that you sometimes hear are like, persisters and desisters around childhood. So, there is a body of data that comes out of the seventies and eighties, primarily out of Toronto and Ken Zucker’s clinic that asks the question...how many boys who are wanting to wear dresses in childhood go on to be trans identified. That’s the real question, right?..If you were assigned male at birth and you wanted to play with dolls and act effeminate and then you didn’t want to do that, sort of in adolescence you are considered a desister. And if you have a gender identity of something different than male you are considered to be a persister. It’s not my language I hate it, I think it’s horrible…So that data that showed well you know most of the people who are assigned male, they were boys who wanted to wear girl’s cloths, actually anything but…. (audience member they were boys who wanted to wear girls’ cloths). Exactly!
1) Olson-Kennedy “hates” words that are merely value neutral descriptors.
2) She downplays desistance by saying they just were boys who wanted to wear girl’s clothes.
And:
…The issues around this particular body of data is…the question is different, and how you measure gender dysphoria is different, and what the follow up time period is, is different, the nature of the fact that the clinic kind of practiced a reparative model impacts the data. So, there is a lot of stuff that makes it not very useful in many, many ways. Except as a tool against the community.
The argument here is children who desist are harmful entities to trans people, and thus, everyone should avoid discussing their experiences. She frames concern for them as a "tool against the community," and they should prevent centering information regarding children who outgrow gender dysphoria to "protect trans people." This has become mainstream among affirmative model advocates and liberal media outlets. This is just one example of many cases of censorship occurring around discussions about increasing numbers of minors seeking medical transition services.
In the following quote, they argue that it is better to subject trans youth to medical consequences and potentially mistakenly transition a would-be gay/lesbian child than to have the youth experience discomfort in puberty and miss an opportunity to "pass" better. They'd have to demonstrate the benefits outweigh the costs, which they have not. For more discussion on the pros and cons, see moral dilemmas.
Here, an audience member at a Q&A for mental health and medical professionals at a Gender Odyssey (2017) conference frames worrying about minors undergoing castration, mastectomy, and hormonal body modifications that were ultimately unnecessary as "cis sexist":
Julia Serano who’s a trans academic who a lot of people have heard about. And scientist, has a fantastic article where she discusses this in great detail. And the concept that she brings up that I feel like we are kind of talking about here and that I want to make sure is centered here is, she talks a lot about how, the fact that we live in a culture that values trans bodies less than cis bodies. And that that is the foundation of where a lot of this fear comes from. Like there’s a cis woman who wants breast reduction, breast augmentation and they are on the autism spectrum, they have a psychotic disorder. They have borderline personality disorder or bipolar disorder or anything like that. These conversations are not so fraught. You can have the surgery. It may be a mistake. It may not be a mistake. You may regret it. You may not regret it. You may like the results, you may not. But the fear seems to be this good cis body is going to turn into a less valuable trans body if a mistake is made. I think that that underlying cultural fear is an important thing to hold and interrogate when we are asking these questions…the author is Julia Serrano...it (the article) was about detransitioning and like children…I mean the big fear was around children who transition and regret it later. That was what the article addressed… children transitioning and the big fear was about children who transition…
She then goes on to frame this article about detransition as “transphobic. The article is balanced, and nowhere does it say people should not transition. Any conversation about desistance or detransition threatens the adoption of early social and medical transition.
Gender dysphoria experts who acknowledge desistance

Not all mental health and medical professionals downplay desistance statistics. Some are alarmed affirmation protocols could track some youth who would have naturally aligned with their biological sex for a medicalized pathway instead. Some of these people work in mental healthcare, like Dianne Ehrensaft, the most outspoken early social transition supporter.
A quote from the research paper, “Gender Identity Disorders in Childhood and Adolescence Currently Debated Concepts and Treatment Strategies”:
Only 2.5% to 20% of all cases of GID in childhood and adolescence are the initial manifestation of irreversible transsexualism. The current state of research on this subject does not allow any valid diagnostic parameters to be identified with which one could reliably predict whether the manifestations of GID will persist, i.e., whether transsexualism will develop with certainty or, at least, a high degree of probability. The types of modulating influences that are known from the fields of developmental psychology and family dynamics have therapeutic implications for GID. As children with GID only rarely go on to have permanent transsexualism, irreversible physical interventions are clearly not indicated until after the individual's psychosexual development is complete. The identity-creating experiences of this phase of development should not be restricted by the use of LHRH analogues that prevent puberty.
In a reply to the Temple Newhook et al. (2018) article which criticized desistance stats and the watchful waiting model, Steensma protests the innate hard-wired gender viewpoint in favor of recognizing developmental psychology and the reality of gender identity change in children:
We agree that the longitudinal studies currently available have their limitations. We do, however, strongly disagree with the authors that studies on gender variant children's development should be abandoned and that our studies do not take children's needs and voices seriously or are unethical.
Jesse Singal commenting on the Steensma study:
Set aside all the noise, though, and the usual caveats about not overextrapolating from one study: The key question is whether for a significant percentage of kids, gender dysphoria abates in time. All the available evidence we have, limited though it may be, suggests it does, and reinterpreting Steensma (2013) in a more accurate light makes the case a bit stronger. WPATH and the American Psychological Association and the Substance Abuse and Mental Health Services Administration and the Endocrine Society all recognize that desistance occurs, and I have never spoken with a clinician who believes it to be a full-stop myth. There is good reason for this expert consensus.
Ken Zucker makes the point that some gender dysphoria professionals who support the affirmative model seem to actively dislike the fact that research shows some children outgrow GD and want to suppress it:

Richard Green, one of the most experienced psychiatrists with a long history of working with GD patients, acknowledges the reality of desistance in youths with serious gender dysphoria, has this to say about dismissing GD:
Caveat, in assessing studies, caution is required in dismissing the reportedly gender dysphoric children who do not persist with gender dysphoria as those who were not genuinely gender dysphoric. This is the circular reasoning of the no true Scotsman fallacy…
Not all gender specialists agree with Dr. Spack, quoted in this article as wanting to lower age of consent laws for medical treatment of minors:
When I subsequently speak to Dr. Polly Carmichael and members of her multidisciplinary team at the Tavistock, it is clear they do not share the conviction that diagnosis for prepubertal children can be so straightforward. Carmichael says that because the treatment pathway identified by Spack is relatively new, “We don’t honestly know and, in fact, you can’t know the longer-term outcomes of these decisions.”
Jack Drescher is another psychiatrist who believes desistance is real, and that the affirmation model may affect the likelihood of desistance, also finds this is an issue of ethical consideration:
There are mental health professionals in the U.S. who agree. Dr. Jack Drescher is a clinical professor of psychiatry at Columbia University; he served on the American Psychiatric Association's committee that revised the diagnosis of gender identity disorder in 2013. He said gender affirmative therapists have never proven they can successfully identify those kids who will stick with transgender identity.
Dr. Susan Bradley is a professor in the Department of Psychiatry at the University of Toronto and has seen over 400 cases of children and adolescents with gender issues. She states in an article titled “CBC Self-Censorship Part of Frightening Gender Identity Trend”:
The reality is, however, that there is no credible evidence that the affirmative approach is effective or safe, a key construct in accepting interventions in medical practice today; nor is there a scientific marker for a ‘true” trans or for a desistor. As was noted in the BBC documentary by GIC researcher Dr. Devita Singh, in a study of 100 boys who attended the GIC, 88 desisted post-puberty, even though their childhood certainty had been as intense as those who persisted.
We did not deny hormone treatments, prescribed by informed endocrinologists, where no other option seemed likely or safe, but continued to monitor their progress for safety, inasmuch as we could, given the lack of scientific knowledge regarding long-term impacts. Still, we favoured postponement of irreversible treatment until it was absolutely clear there was no chance of desistance. For observing this cautionary principle, we are often vilified as “transphobic” by activists and ill-informed sympathizers in the general population.
Polly Carmichael in a presentation (39:59-40:20) on adolescent mental health in response to a concerned mental health counselor:
I’m with you. These are very difficult challenging issues and I guess we just don’t have enough evidence. There is obviously a worry that by introducing certain things, such as earlier treatments, you are in some way changing the outcome of those things
Sasha Ayad, M. Ed., LPC, believes in a mental health counseling approach rather than merely an affirmative approach to trans identified teens:
Just as Vanderburgh has seen talk therapy as an effective treatment for dysphoric post-transition clients, I have also seen benefits of therapy for pre-transition clients. Trans-identified teens can and do experience a reduction, if not elimination, of gender dysphoria through talk therapy. Many of my clients have desisted in the context of support, respect, and careful exploration. Rather than take their feelings of incongruence at face value, we explore deeper messages signaled by their body-discomfort. Next time you hear that “desistance is a myth”, recognize the phrase as another misinformed and manipulative slogan used to pathologize (and medicalize) the bodies of trans-identified kids…
Our go-to approaches must be those which are least disruptive and least risky. We must carefully study the impact of various types of psychotherapy on ROGD teens. We must remain scientifically grounded and morally watchful when dogmatic political agenda takes the place of ethical, compassionate care. The incoherent philosophy of “innate gender identity”, which underlies “affirmation” is not scientifically, psychologically, or philosophically sophisticated. At best it’s lazy and superficial, and at worst, it plays an iatrogenic function, creating pathology – and a life-long medical patient – out of thin air.
In reality persistence/desistance is complicated as summed up here by sexologist James Cantor:
Importantly, these results should not be exaggerated in the other direction either: The correct answer is neither 0% nor 100%. Although the majority of transgender kids desist, it is not a large majority. A very substantial proportion do indeed want to transition as they get older, and we need to ensure they receive the support they will need. Despite loud, confident protestations of extremists, the science shows very clearly and very consistently that we cannot take either outcome for granted.
“I am a girl” versus “I wish I was a girl” presented as a way to soundly diagnose “true trans” children
There has been a recent effort to promote the idea that if a female child says, “I am a boy” versus “I want to be a boy,” then that child is trans and will stay trans.
Kristina Olson released a study on trans-identified youth that showed that when given a gender identity test, these youth look like opposite-sex controls. The implication may be that “transgender children” identify as trans and show the same stereotypical interests as “cis” boys and girls and, thus, should be affirmed in their stated gender:
Using implicit and explicit measures, we found that transgender children showed a clear pattern: They viewed themselves in terms of their expressed gender and showed preferences for their expressed gender, with response patterns mirroring those of two cisgender (non-transgender) control groups. These results provide evidence that, early in development, transgender youth are statistically indistinguishable from cisgender children of the same gender identity.
However, there are some issues with the way they present these results. Notably, they defy the clinical experience of several gender experts who found that some seriously dysphoric, opposite-sex identified youth (even youth with an “aversion to their genitalia”) outgrow dysphoria. Kristina Olson’s definition now defines such children as “transgender children.”
In the graphic below, we see children diagnosed with gender identity disorder indeed desisted in some cases. Some of the diagnostic criteria were different than DSM-V, but it is reasonable to believe these numbers contain youth who were cross-sex identified at one point. It is also apparent that some youth who don’t have a DSM diagnosis in childhood decide they want to transition as they get older (around 10% averaged across four studies). So “I am a” is likely a better indication of the severity of the child’s gender dysphoria in the moment rather than a clear screening tool:


Ken Zucker USPATH presentation 2017
Reporter Jesse Singal makes the following observations about Kristina Olson’s study and how her definitions are misused by important medical governing bodies like the AAP, which now references it in its policy statement:


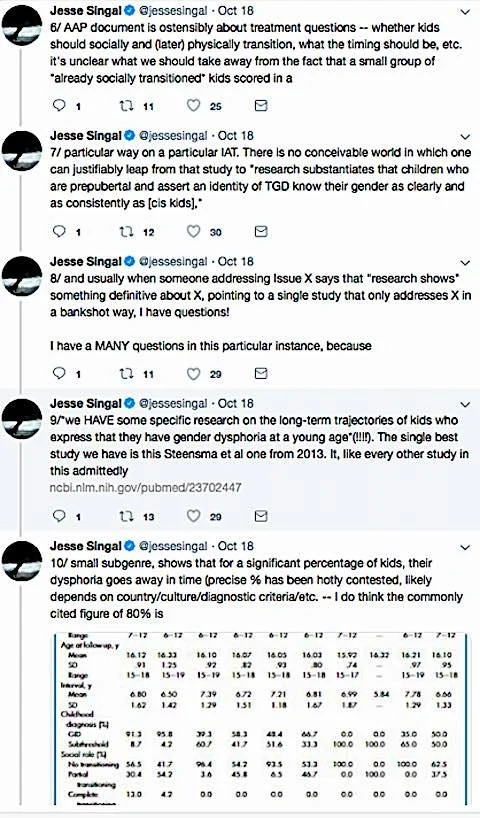
Affirmative model skeptical site 4thwavenow makes some interesting points (it’s worth reading all of them) in this blog post about Kristina Olson’s assertions:


Kristina Olson has recently made comments in the press that tell the public socially transitioned children are trans because they say they are and exhibit behaviors and interests of the opposite sex:
By studying the 85 gender-nonconforming children she recruited, her team has now shown, in two separate ways, that those who go on to transition do so because they already have a strong sense of their identity.
However, her research does not discredit desistance or prove that less drastic means are ineffective in helping youth manage or overcome gender dysphoria. It only states the obvious: more dysphoric children are more likely to transition socially; highly dysphoric children are likely to be more gender-nonconforming than desisters. The paper reinforces its argument with many colored graphs demonstrating dysphoric children match gender stereotypes. The problem is that many gay and lesbian people strongly align with cross-sex stereotypes as well. For evidence of this, see here. Gay men involved in ”ball culture” are often more feminine than the average female, even when they aren’t in drag. This kind of cross-sex behavior is well understood in the gay and lesbian community. Lines between gay and trans can be very blurry despite an activist-motivated narrative that describes gender identity and sexual orientation as separate phenomena:

The other issue with the study is that the children were affirmed as trans by their parents at times from very young ages. Some are prepubertal children, and doctors are likely to prevent exposure to normal hormonal processes right at the beginning of puberty. A normal puberty may facilitate the resolution of GD due to exposure of sex hormones in the brain. It seems reasonable to consider developmental psychology effects or the powerful effects of hormones on the body.
It is worth noting that Dr. Ray Blanchard, one of the world’s experts on adult gender dysphoria, does not think “I am a” versus “I wish I were a” is a solid way to diagnose adults, much less children. Children do not understand themselves as well as adults and are not cognitively mature:

Steensma, one of the most experienced scientists in gender dysphoria treatment and research, criticizes Ehrensaft’s assertion that she can diagnose a trans child based on the “I am a…” criteria:
“(E)xplicitly asking children with GD (gender dysphoria) with which sex they identify seems to be of great value in predicting a future outcome for both boys and girls with GD,” the study says.
Today, Steensma cautions that this question is not a litmus test for which children will persist in their transgender identity. He believes that gender identity in kids is still developing, and that it’s responsive to what occurs at different life stages. He also says it’s possible that a social transition could lead to persistence where it otherwise might not have occurred.
Dr. Singh does not seem to support “I am a” as diagnostic:
Credulous establishment figures have bought into this narrative, which is now firmly ensconced in our educational, medical, social service and legal institutions. The reality is, however, that there is no credible evidence that the affirmative approach is effective or safe, a key construct in accepting interventions in medical practice today; nor is there a scientific marker for a ‘true” trans or for a desistor. As was noted in the BBC documentary by GIC researcher Dr. Devita Singh, in a study of 100 boys who attended the GIC, 88 desisted post-puberty, even though their childhood certainty had been as intense as those who persisted.
Any assertion that all children who say they are trans have an “innate” and “deeply held” gender identity impervious to change may be a hasty conclusion. While people do this all the time in everyday conversations, in this case, scientists are framing the discourse around protocols that lead to irreversible medical treatments on children:
Hasty generalization is an informal fallacy of faulty generalization by reaching an inductive generalization based on insufficient evidence—essentially making a rushed conclusion without considering all of the variables. In statistics, it may involve basing broad conclusions regarding the statistics of a survey from a small sample group that fails to sufficiently represent an entire population.[3] Its opposite fallacy is called slothful induction, or denying a reasonable conclusion of an inductive argument (e.g. "it was just a coincidence").
Even pro-affirmative model advocate Erica Anderson admits children who are saying “I am a girl” may not have done so in the past. Here, Anderson talks about how now, children embrace a trans identity they may not have had several years ago:
We’ve got kids of varying sophistication levels of language trying to explain to other people who have no experience [being transgender]," Anderson said, "and it’s being driven by shifting professional understanding or consensus and culture. You’ve got moving parts. In that context we’ve got a dynamic situation where kids who might say ‘I’m a girl’ might have said five years ago ‘maybe I’m a girl.’
F. Obscuring the link between gender dysphoria & adult homosexuality / bisexuality
Activist Dana Beyer provides an example of the viewpoints of some in affirmative model circles by emphasizing the benefits of social and medical transitions for dysphoric youth while minimizing the possible adverse effects on dysphoric desisters:
If one follows the Hippocratic system and prioritizes doing no harm, the priority must be to transition the trans girls and not worry as much about the inadvertently transitioned gay boys.
Trans activists and allies have published similar articles in the Huffington Post, ThinkProgress, and other liberal publications. While positioning arguments for one’s community is understandable for any activist or human being in general, this attitude becomes more problematic when it is held by doctors and therapists working with dysphoric youth, given the reality that some dysphoric youth outgrow GD and are very likely to be LGB as adults. Citations confirming the link between childhood gender dysphoria and adult homosexuality can be found here. The connection between gender dysphoria and bisexuality is becoming more of an issue with increasing numbers in trans-identified teens claiming a bisexual orientation.
The public comments made by pro-early medical transition professionals indicate they are not concerned about misdiagnoses. This is problematic because there isn’t a clear line between trans people and very gender-nonconforming homosexuals. An effort to separate children into these neat categories so protocols appear more scientific and safe will likely fail. It is already starting to harm homosexual youth.
Gender dysphoria & its connection to adult homosexuality or bisexuality
For a discussion of research data on childhood GD, desistance, and evidence of high rates of LGB adults among those who outgrow GD see here. It appears the rate of same-sex attracted desisters may be as high as 50%. However, many lesbian and bisexual females do not come out until their twenties, so follow-up responses to sexual orientation may later change. It is also possible that more seriously dysphoric children are more likely to grow up to be gay men or women than a less dysphoric cohort. Previous studies indicate children with GD who transition as teens are almost all homosexual males or females, although the demographics are changing rapidly.
Here, Polly Carmichael, a youth gender dysphoria expert states:
The available evidence suggests that most prepubescent children with gender dysphoria will have a different outcome in adulthood, Carmichael says: ‘The most common would be one around sexuality, rather than gender identity.” In her experience, they are more likely to be LGB than T.’
Carmichael is not the only gender dysphoria expert who acknowledges the blurry line between gender nonconforming, likely pre-LGB youth, and trans youth:
Gender fluidity is common among children, but it typically crystallizes during the teenage years. Among preadolescents who manifest GID traits (meaning serious dysphoria), 80 percent will “desist” from being transgender before entering adolescence, according to Kenneth Zucker, Ph.D., of the University of Toronto. Half or more of the youths will go on to identify themselves as gay or lesbian.
And from “A follow-up study of girls with gender identity disorder” (2008):
At the assessment in childhood, 60% of the girls met the Diagnostic and Statistical Manual of Mental Disorders criteria for GID, and 40% were subthreshold for the diagnosis. At follow-up, 3 participants (12%f) were judged to have GID or gender dysphoria. Regarding sexual orientation, 8 participants (32%) were classified as bisexual/homosexual in fantasy, and 6 (24%) were classified as bisexual/homosexual in behavior. The remaining participants were classified as either heterosexual or asexual.
In Korte et al. (2008) the researchers express that hormonal therapy may interfere with the youth’s formation of a homosexual identity:
Experience has shown that, in not a few cases, a strongly and resolutely asserted desire to change to the opposite sex becomes markedly neutralized over the course of time, and the individual later undergoes a homosexual "coming-out" (1, 3). In view of this fact, it must be understood that early hormone therapy may interfere with the patient's development as a homosexual. This may not be in the interest of patients who, as a result of hormone therapy, can no longer have the decisive experiences that enable them to establish a homosexual identity.
I have met gay women who identify as women who would certainly have been diagnosed gender dysphoric as children but who, throughout adolescence, came to accept themselves. This might not have happened on puberty blockers.
Many homosexually attracted people themselves talk about having been gender dysphoric as youth. Anecdotally, here is a quote from model and actress Ruby Rose:
Rose, who came out as lesbian at age 12 and identifies as gender fluid, said previously that she had started saving money for the surgery, but eventually decided against it.
I had this jar that I would collect dollars – in fact, we were so poor, it would have been cents. So I probably had 19 cents to go towards this surgery that I didn’t really know a lot about. I think I had seen like a daytime documentary, probably something on Oprah and I was like, ‘That’s what I’m going to do.’ And so I started saving from probably the age of 5…
I’m a woman … I want to have babies one day, so I’m glad I didn’t make changes earlier in my life.
And this gay man:

“Terry Patterson is a Student Counsellor, Trainer and Clinical Supervisor for university counsellors and previously managed a large university counseling service in London for 14 years.” As a college instructor, she became disturbed by the large numbers of trans identified females in her classes who, in the past, all identified as lesbians:
I was one of those children who ‘felt like a boy’, preferred boys clothes, loved football and my racing bike. It was distressing to find myself attracted to girls and if I’d been born 40 years later than I was, I may well have labelled myself as trans and gone down the route of changing my gender. This is also true of most gay, lesbian and bisexual friends, colleagues and clients I’ve talked to over the years. Perhaps we were fortunate to have been children in an era before the polarisation of gender became a global industry. We are all now ordinary, and some quite extraordinary middle-aged people who are comfortable in our identities, and proud of ourselves for surviving the painful process to get there. It’s worth remembering that a number of recent research studies have concluded that most children who are gender non-conforming grow up to be happy gay men and lesbians (Drescher & Pula, 2014).
More anecdotal examples below:
I guess reading about trans kids hurts so much because like… that would’ve been me. at six or seven, when i was sobbing at the thought of having to wear pink? at twelve or thirteen, when i was so deeply ashamed of my period and would’ve given anything in the world to get rid of it, when i was purposefully cutting my hair and experimenting with my clothes to try and pass as a boy in public, fantasying about someone calling me ‘him’? that would’ve been me. like, maybe it goes deeper than “playing with barbies or trucks”. maybe the trauma of girl children and gay children is deeper than that. i didn’t know i was gay until i was almost seventeen years old. i could’ve been on hormones for years. i could’ve had top surgery. if i had been born ten years later and my parents had been informed enough to notice the patterns in my behaviour, if medical intervention had been a real option, i would’ve been living as a boy before i knew so many basic fundamental truths about myself, such as that i love women…

Warning: graphic

These videos were submitted to USPATH for their 2017 seminar and are by detransitioned lesbians. Dr. Olson Kennedy, Diane Ehrensaft, and many other pro-early transition gender specialists attended this seminar.
Video for USPATH Max
Video for USPATH Cari
When people downplay the connection between trans and gender nonconforming LGB, it makes a complicated situation seem simple in the minds of the public, the minds of the therapists and medical professionals they train at gender seminars, and in their own minds. One possible explanation for transgenderism, homosexuality, and bisexuality is that it is a result of in-utero hormones, although how is not clear. If this is the case, these influences are likely on a continuum with no clear line between populations and no way to determine where that line is in children or how culture and social transitions will affect this. There are people in the middle, both adults and children, for whom extreme medical intervention is not the best solution. Adults will not give these borderline young people alternative coping strategies under the gender affirmative model. There are already examples of harm or near harm resulting from this reality.
Affirmative model advocates seeming to avoid discussion of the connection between adult homosexuality & childhood gender dysphoria
There have been several examples of trans activists saying they want to distance themselves from the homosexual rights movement to make advocating social transitions of young children more palatable to schools and the public in general. Fox Fisher (Gendered Intelligence-Britain) mentions it in a now-deleted video that may have been removed because many people complained on social media that this claim was anti-gay. Joel Baum (UCSF, Gender Spectrum, California) at a gender conference:
Joel Baum (39:15-41:17):
The third dimension then is gender identity. Now you’ll notice I’m talking about these three dimensions, I don’t Believe I’ve said the word lesbian, gay, bisexual, asexual, pansexual, omnisexual or any other kind of sexual. And that’s because those are all terms related to sexual orientation. And sexual orientation and gender again are not the same thing. Is there any relationship? Sure, but they’re not one in the same. I mean think about it for a second. Sexual orientation in many ways is understood in terms of my experience in relationships to others. Gender on the other hand is very much my own experience of self. My experience of who I am. And it’s problematic to confuse them for a couple reasons. One is we frequently read a young person’s expression and assume it tells us lots of stuff about their identity. And in fact, you know I was a couple of weeks ago doing a presentation for some early childhood educators and one of them raised their hand and said, “What am I supposed to do with the parent, usually a dad, who comes in and says I do not want my son playing in the dress-up corner. I do not want a little gay boy on my hands. I’m just not gonna’ have it. Not gonna’ have it. What I’m I supposed to say.” And I’m like well, first of all it’s your preschool by the way and you probably have enough on your hands worrying about keeping the kids safe then what they’re playing with. But also, you know, that kids three I think. Could we just give him a minute to figure out the attraction stuff and just let him play? Right?
But more importantly, when we confuse sexual orientation and gender we put a very adult lens of sexuality on top of the process of identity development that just is not on the table. So, when we think about supporting transgender young people in our schools and restrooms and our locker rooms on overnight field trips, and housing accommodations, many people’s minds go straight to sex and a sexually loaded situation. When in fact it’s not about that. It’s about identity. And the issue is not who’s going to have sex with who but who is going to be honored for who they are.
While almost everyone believes that small children don’t need exposure to concepts around their sexuality, there are multiple reasons why gays and lesbians and other pro-LGB people who follow this issue find these types of statements coming from affirmative model advocates concerning or offensive.
1) Joel Baum acknowledges societal homophobia and appears to want to distance the trans movement from it to affirm small children as trans.
2) It seems to present trans identity as non-offensive enough to discuss in schools. It frames homosexuality as inappropriate to discuss even though it is true many gender nonconforming and even dysphoric youths are pre-LGB and not transgender. Baum paints the concept of understanding a very effeminate male child may likely grow up to be gay (with a healthy, non-medicalized body) as looking at them through a ”very adult lens” and taboo. And conversely, he enthusiastically reinforces a child’s gender dysphoria.
This form of affirmation increases the odds of a medicalized path. Under this model, the boy in Baum’s example risks destroying the functioning of his sex organs, fewer choices about bottom surgery, sterilization, and potential negative cognitive and long-term health consequences. Yet these outcomes are somehow less “adult” and less taboo? This attitude exists in the extreme in Iran, where gay men and lesbians are forced to transition medically or else they will receive the death penalty. Transsexualism is less offensive to Iranians than homosexuality.
In short, one interpretation insinuates a gay child is more taboo than encouraging a medical pathway. Some LGB people see this as an invitation to set up a medical transition paradigm for GNC children.
3) Many LGB people find it concerning to affirm the identity of dysphoric youth who are too young to understand their sexuality and understand that other people, particularly gay men and lesbians, have felt the way they do but evolved into an adult gender nonconforming sexual identity without medical modification.
A gay man who felt dysphoric as a boy himself (even “tucking” at times) speaks to the trans activist tactic of distancing themselves from homosexuality to promote gender identity and how this is a point of skepticism. Below is one explanation of why many LGB people feel this movement will be confusing to borderline GNC youth too young to understand their sexuality and will play into societal and internalized anti-gay, bi, and lesbian sentiments:

In a piece for Quillette, Debra Soh, who is a heterosexual neuroscientist, echoes this same concern in “The Unspoken Homophobia Propelling the Transgender Movement in Children”:
And as I’ve watched as glowing stories about transgender children have flooded every progressive news outlet over the last few years, every one of them appalls and saddens me. Because the underlying story that the public isn’t privy to is that many of these children would have grown up to be gay, but are instead undergoing a new form of conversion therapy…
Children will say they “are” the opposite sex because that’s the only language they have to express to adults that they want to do things the opposite sex does. Cross-sex behavior has also been shown to be a strong predictor of homosexuality in men. Previous research tells us that even children who are severe in their feelings of dysphoria will desist.
4) They don't acknowledge desistance and how children with a pre-LG orientation may outgrow GD or how this reinforcement of gender identity, painted as non-offensive (unlike sexuality), will affect them.
5) It trivializes gay, lesbian, and bisexual identity and its long history of pushing gender norms by framing it as just something you "do" rather than the more deeply held something you "are.
6) Sexual orientation in trans, homosexual, bisexual, lesbian, or heterosexual youth is dismissed as relevant here. Sexual orientation is a pertinent issue in talking about showers, locker rooms, and sleeping accommodations (all situations where trans activists want youth placed based on gender identity alone). Suppose a 17-year-old biological male MtF who is attracted to girls is placed in a locker room or sleeping accommodation with girls. In that case, this violates girls' privacy rights and is a liability issue for the school. Not all MtFs are attracted to boys/men, and the ones who are attracted to women appear to be coming out at younger ages. A more in depth conversation about conflicts of rights and the trans movement can be found here.
It is true that a few people critical of medical transition view trans people as “self-hating gay people” or as people transitioning to fit into gender norms because of anti-gay attitudes in society. While there is some evidence that homophobia can influence youth to identify as trans, most trans people don’t say they feel this way and view themselves as the opposite sex. Criticizing this viewpoint for them is understandable. But what is questionable is that the affirmative model denies that there is any link at all between homosexuality and gender dysphoria. There is too much desistance information to ignore the connections between the two. There are also many personal accounts of gay men and lesbians who say they had gender dysphoria to varying degrees, as well as many desisters and detransitioners who re-identify as gay, lesbian, or bisexual once their trans identification subsides.
Dr. Johanna Olson-Kennedy (Gender Odyssey, 2017):
I like how transgender people don’t see themselves as gay when they obviously are, as in like it, I mean I hate it. Because they are a group of liars.
This statement is reasonable for adults who are attracted to their biological sex and who don’t see themselves as gay or lesbian but transgender. However, the link between childhood gender dysphoria and adult homosexuality is well-established. This statement was made in a discussion about children and hormone blockers at a five-day seminar where, in many of the workshops, there was zero discussion about the risks of an affirmative model, the potential for desisters, or the developmental and psychological effects many might face if they are socially transitioned and given hormone blockers at young ages.
Are doctors morally obligated to consider all possible outcomes and all of their patients' safety? Olson-Kennedy could make a similar statement: "I like how affirmative model advocates act like there is this clear line between a trans child and GNC pre-gay or lesbian child coping with GD, as in like, I hate it. Because they are a group of liars." There is evidence of harm to gay and lesbian youth inflicted by the medical transition industry (cases recorded in Britain and Thailand), desistance data, clinical observations of dysphoria experts, and gays and lesbians who feel these protocols could have hurt them as children, and desisters and detransitioners who are now gay and lesbian identified people.
Again Norman Spack:
People tend to confuse sexuality and identity, and often want to conflate these things, but being transgender has nothing to do with sexuality. And there are still those who feel that because 60 to 80 percent of kids who act in a cross-gender way aren’t in fact transgender, that we shouldn’t be encouraging this. This is one of the big debates.
This is an odd assertion since he acknowledges a dysphoric pre-tanner stage 2 child may in fact be a pre-gay child.
Prior to tanner 2 we cannot be absolutely, absolutely! sure whether a child who affirms the opposite gender will indeed remain so and not just become gay or lesbian or gender variant in other ways.
Here is a quote from Dr. David Schwartz assessing bias and lack of concern for gender dysphoria desisters from this article in the Journal of Homosexuality:
Given this uncertainty of prognosis, it is significant that Edwards-Leeper and Spack’s presentation of the pros and cons of pubertal suppression, a primary intervention in their protocol and their frequent recommendation following diagnosis, is imbalanced. They offer seven physiological benefits to pubertal suppression (for the most part just a list of the physical effects) and no disadvantages. Likewise they tout the psychological advantages, but note no potential disadvantages.
Diane Ehrensaft downplays what many people consider an obvious connection between same-sex attraction and childhood gender dysphoria (1:10:57-1:11:05):
Let me repeat what Joel sad, Gender development and sexual identity development are two separate tracks
She repeats this here in this journal article:
It is also recognized that gender development is a discrete and separate track from development of one’s sexual identity.
But in some cases, they are likely not “two separate tracks” but are the same biological effects on a severity spectrum that culture may influence. Ray Blanchard has shown that male birth order is correlated with both male homosexuality and MtF transgenderism, indicating that these factors in determining each identity aren’t “separate.” This is a reality many people who exist in LGB populations are aware of simply because of life experience (experienced GD, had partners with GD, have gender-bending gay and lesbian friends, etc.).
Saying gender identity and homosexuality have “nothing to do with each other,” given that most young females and males who medically transition are same-sex attracted (biological sex), just as gay men and lesbians are, is an ideologically expedient argument.
Here, Diane Ehrensaft appears to believe that there is no reason to worry a dysphoric pre-homosexual youth could experience consequences, confusion, or trouble changing their mind after spending the entirety of their childhood being reinforced in their gender dysphoria and living as the opposite sex. The quote below is also an argument from ignorance, not a statement of scientific fact. Anecdotally, there are growing numbers of young people desisting and detransitioning, and some describe the experience as traumatizing:
The stress [of detransitioning] comes from microaggressions and lack of acceptance in the environment,” she said. “If we offer social support and opportunities for children over time, we don’t have any evidence that [detransitioning] will be damaging for them.
Kristina Olson and Lily Durwood from the Trans Youth Project are quoted below from a piece that de-emphasizes concern about early social transitions and its possible effect on borderline GNC youth (emphasis theirs):
This is not to say that a transgender identity in childhood never desists in adulthood. The truth is that we do not know precisely how many transgender children will grow up to be transgender adults, because no long-term studies have recruited a large number of children who believe that they are members of the opposite sex nor separated the few they have included in past studies from the broader group of gender nonconforming children…
By systematically studying the impact of social transitions in transgender children, and by studying outcomes in transgender children whose families make a wide array of decisions, we can best discover what is in the best interest of the transgender child.
1) Olson and Durwood are already labeling and affirming gender dysphoric children as “transgender children” without a developmental psychology discussion or reference to other gender clinicians or studies that observe culture and environmental influences and their possibility to increase persistence.
2) The assertion that the previous studies weren’t accurate enough to determine levels of desistance may be questionable as previous studies show high rates of desistance, even among children diagnosed with gender identity disorder. DSM-IV and DSM-III were less stringent criteria than DSM-V but still involved the child being distressed. Viewing all these children as merely gender nonconforming is debatable.
3) These points, and Olson and Durwood’s Slate piece in general, seem to indicate a total and complete lack of concern or intellectual curiosity about what type of mental health and identity formation support a pre-gay or lesbian child may need to make a non-medicalized adjustment into adulthood. Olson and Durwood do not mention the word gay or lesbian once in this article. Why? Are they emulating Joel Baum’s view that bringing up homosexuality and dysphoric youth is taboo? Are they being influenced by trans activists who don’t want homosexuality brought up in these discussions at all? Are they intentionally avoiding discussion of the risks this represents to the gay and lesbian community to facilitate child social transitions that will most likely lead to hormone blocker use at age ten or eleven? Or is it apathy towards other communities (LGB, autism spectrum) outside of the trans community that could be negatively impacted by affirming protocols?
4) Olson and Durwood characterize all concerns as “alarmist” in this article, seemingly unable to absorb how unethical it would be to track any GNC youth into hormones and surgery based needlessly on decisions they made as children. The consequences of the inappropriate transition of a minor are extremely serious and worth considering.
Desisters were really closeted trans people
Another narrative promoted by both trans activists and affirmative model professionals is that people don’t desist from gender dysphoria and often adopt gay or lesbian identities, but that desisters and detransitioners are really still trans, and they detransition only because of transphobia. Julia Serano states this. While this may be the case in some situations, it is a denial of reality to ignore desisters and detransitioners who reject their previous trans identification. Many detransitioners find this denial of their stories offensive (see here and here and here).
Jack Turban, a psychiatry resident at Harvard, thinks parents should believe “It’s no big deal” if their minor children medically transition and regret it later. He provides an example of the new, very pro-medical transition and social affirmation attitude permeating universities. He is a writer for Psychology Today and says this:
Affirmative model advocates promote this argument in Temple et al. 2018, a journal article Thomas Steensma and Ken Zucker criticized.
There is no substantial evidence that the majority of desisters “went back in the closet.” Many studies and clinical observations of dysphoric youth come from liberal countries with a tolerance for trans people and a public healthcare system to help pay for treatment that young adults who were still trans would likely access. This comment is also ignorant of the fact that a large portion of desisters are likely to be gay, lesbian, or even bisexual (females especially). Tolerance for homosexuality isn’t necessarily higher than for transgenderism. In Iran, the government tragically forces gay men and lesbians to medically transition to correct their “deviant” homosexuality, which is against Islamic religious beliefs. Legal transgender identity change is possible in more conservative Islamic countries than same-sex marriage. This is one of the significant concerns gay and bisexual people have around youth transitions and how it could be used to “correct” gender nonconforming, likely pre-LGB children.)
There are accounts of gender clinicians observing parents making comments such as, “at least ‘she’s’ not gay.” Bernadette Wren and Ken Zucker have made comments that do not support Turban’s argument. Being a butch lesbian or an effeminate gay man isn’t easy in society and isn’t always even easy within “the community” itself. A young lesbian sums up the reality of the difficulty in being a gender-nonconforming gay man or lesbian on her blog:
It’s better to be a cute boy than an ugly butch lesbian.
Jack Turban is a gay man, so his reasoning is odd and contrary to what the research says. He has most likely heard of this phrase, “no fats/ no femmes,” which is something effeminate gay males trying to date frequently see on gay dating apps. Some MtFs have stated they transitioned because they thought they would have an easier time with straight men than gay men because they were so feminine and the gay male world worships masculinity. “Faggot,” “sissy boy,” “limp wrist,” and “poofter” are not positive words and do not express a supportive environment for effeminate gay males. Society also has very negative views of butch women, who have zero positive representation in pop culture. These realities do not bolster the argument that these desisters aren’t gay but trans-closeted because gays are supposedly treated so much better than trans people. This FBI report on gay and trans bashings seems to indicate gay people are more at risk. Transphobia and homophobia are both realities. In some cultures, one is worse than the other. In other cases, it’s the reverse or the same
Gay people have said they were dysphoric children and outgrew it. And this study shows the opposite of what Turban is saying. It’s not that transphobia fuels a homosexual identification, but instead, homophobia fuels a trans identification.
In the below quote, Steensma (who ran a study showing high numbers of desisters), debunks the “transphobically oppressed desister” argument:
Parents who come to our clinic are concerned about potential harm for their child if they would not acknowledge the child's gender experience. They are not focused on suppressing it, as the authors suggest by the sentence:
Furthermore, even within Toronto and the Netherlands, this research was limited to children whose parents chose to bring them to a clinic for diagnosis and treatment and thus may have believed the child's difference was a problem, and one that required psychological treatment.
Our group is indeed a clinical one, but not all clinical groups are characterized by a suppressing attitude of their environment. We feel that, besides the unfounded assumptions that are made by the authors about the intentions of the supporting and caring parents we see in our clinic, the difference in social context is not properly taken into account in the paper, and that the conclusions that are drawn from our follow-up studies cast a very negative shadow on our clinical approach and the intentions of professionals in our clinic.
For more discussion of homophobia pushing gay and lesbian youth into identifying as trans see here.
G. Statements demonstrating a lack of clear diagnostic criteria
One of the big concerns skeptics of the child medical transition movement have (a 10-year-old put on blockers is a medically transitioned child) is a lack of consideration for the effect that culture could have on persistence/desistence in the face of lack of evidence for a solid screening process. This concern is summed up well in a Medium piece critical of the current push in trans activism:
Ehrensaft then presents a summation of the ‘gender affirmative’ model that LGBTQI+ organizations are promoting, she is promoting, and oligarchs are funding.
“Basic premises of the gender affirmative model
• Gender variations are not disorders.
• Gender presentations are diverse and varied across cultures, requiring cultural sensitivity.
• Gender involves an interweaving, over time, of biology; development and socialization; and culture and context.
• Gender may be fluid; it is not always binary.
• If present, individual psychological/psychiatric problems are more often than not secondary to negative interpersonal and cultural reactions to a child.
• Gender pathology lies more in the culture than in the child.“[…]Remember, according to the Human Rights Campaign and Ehrensaft herself, gender is stereotypes. This paper is literally saying that sexed body does not match the stereotypes assigned to it; it requires medical intervention to ‘affirm gender’. Despite this pathology being cultural, and acknowledging this fact, Ehrensaft still wants to chemically and physically castrate children who do not conform to ‘gender’.
Apples, oranges, & fruit salad
A good example of the messiness and lack of clarity in the evidence and criteria for socially and medically transitioning young children is found in statements from psychologist Diane Ehrensaft’s lectures. She is one of the main promoters of the “gender affirmative model.” In this model, the child’s gender dysphoria is affirmed without any effort to help the child adjust to the biological reality of their body without medical intervention. Her comments often demonstrate lack of a clear way to know actual long-term outcomes. She says gender is both fixed and fluid and that this may or may not change through life. Conversations about how reinforcing gender dysphoria in children could increase persistence are lacking, except to assuage fears that it happens. None of these concerns are reasons, in her opinion, to try to delay a social transition or delay permanent medical treatments on minors. She speaks of gender in mystical, new age terms (“gender creative,” “gender web,” “apples, oranges, fruit salad,” “double rainbow helixes,” “snowflakes,” “dimensions,” etc.). Yet, hard data to demonstrate sound and safe screening processes are not presented:

Ehrensaft (1:14:04-1:14:50):
Now we also, to get a little Twilight Zoney, we have a 4th dimension. And the 4th dimension is time. So, each individual alters their gender web as they weave together nature, nurture, and culture over time. Which means, it’s fluid throughout development. And I will say going back to the theory, what is true in that theory, by age 2 children can know their gender. And for many people does remain stable because of our gender identity for the rest of our lives but not necessarily…Now the gender web is like snowflakes and it’s also like finger prints.
You gender is not fixed by age 6. We see people who change their gender over the course of their life both in expressions and identity, with no aspersion on their character and with no dents on their mental health. What that means is that gender isn’t fixed at 6. It’s a lifelong process. And it’s not based on the sex assigned at birth. It may be but.
Previously, gender clinicians such as Ken Zucker adhered to what could be called a “transition as last resort model.” The new pro transition clinicians promote what appears to be “transition as first resort model.” The transition as first resort model doesn’t mean they don’t do psychological screenings on children and teens (they do in some clinics, but in other cases, no screening is happening). But it does mean they affirm the child’s gender identity. At the same time, they acknowledge gender fluidity in some youth. No value seems to be placed on helping the child deal with the reality of his/her biology. For other conditions, less drastic measures are alway tried first. There seems to be a lack of interest in how cultural factors may help gender nonconforming youth feel more at ease even though multiple studies show other influences on gender identity beyond “innate gender.” Alternative ways of coping with dysphoria are considered transphobic (discussed previously) but may be beneficial to the child so they can transition a little older (avoiding side-effects such as micro-penis and sterility).
Fruit analogies
Here, and elsewhere, Diane Ehrensaft readily admits that for some people gender identity changes over time. She does not see this as any reason to be cautious with social transitions, hormone blocker use, cross sex hormones, or surgeries on minors. Her diagnostic criteria for diagnosing who should transition is based on who she thinks is an “apple, orange, or fruit salad” (USPATH, 2017):
And a majority of children in the clinical studies have proven to be desisters. The most recent finding evaluating the data is that 63% in the Dutch study turned out to be desisters and the rest persisters. So, here’s the question. How could we possibly sort out the persisters and desisters early in life if some of them change course? And if we can’t how can we allow young children to transition from one gender to another, an option for pre-pubertal children? And why do we care? And the model I work from we care because children have better mental health outcomes if you recognize them for the gender they are rather than the gender we think they should be. And this gets me to apples, oranges and fruit salad. So, when I read the data years ago I thought, ‘I don’t get it. You are talking about apples and oranges here.’ We are actually talking about 2 different sets of kids from early on if we stop and think about it. So, I came up with apples and oranges. But then as time was going on we have a whole other group of kids who are our non-binary, beyond gender kids. So, I had to come up with a third category and that’s our fruit salads. And some people had some objections to using the word fruit given its meaning historically but just as we have appropriated queer as a positive term I’m appropriating fruit, and I like fruit salad.
She continues to explain how therapists can determine the difference between persisters, desisters, and “non-binary” children, but again, even this therapist, the architect of the “gender affirmative model,” indicates these methods may not be foolproof. It is relevant that the designer of the pro-transition model has to admit there are no clear criteria in determining which children will want hormones and surgery and which children would not, if they were left alone as they would have been in the past. To justify early social and medical transition, Ehrensaft often uses words like “typically” or “usually.” She has no follow up thoughts on what will happen to the more atypical youths who may look like persisters but are actually would-be-desisters, or at least would have been in the past, other than to say she thinks it will all work out fine. Aren’t the “fruit salads” at risk?
USPATH, 2017:
Typically this child will say ‘I am a,’ fill in the black rather than ‘I want to be a.’ So, to be or not to be…And I want to say as I go along these are not check list where you go at the end ‘got it you have to meet six of these and you are.’ These are just guidelines. And every child is unique. But this helps us just to get some schematic understanding of the differences in the apples and the oranges and the fruit salads.
Now we go to our fruit salads. I started off with apples and oranges and I realized I have to add fruit salad….. And these are children and adults, it’s a tapestry of self, neither male nor female creative understanding of gender both in identities and expressions. These children typically resist gender boxes. Often live in gender middle grounds. No either or but instead all and any. They often will identify as our agender, pangender, genderfluid, genderqueer, children and youth and recently I would say that the culture thread of the gender web is showing up to be very strong. And opening up the doors for fruit salads. And that children are very influenced by the new notion of gender infinity as we saw in the statistics. That 50% of youth don’t just think there’s just 2 genders. And particularly in adolescence, if we think adolescence in our culture is about identity exploration we have now thrown gender into the hopper for kids to explore their gender. And wonder what that is along with their political affiliation, their religion, etc.
USPATH, 2017:
and it’s not always this way but pay attention to it (in regard to children wanting to cross dress in everyday “girls attire”…
Now we have our oranges. Now oranges are our kids that show up in the child gender research as the desisters and here we come to the verb (sic) that they often do not repudiate the sex assigned to them at birth…but they may say ‘You know I wish I was a. I want to be a, more likely. A large number of these children will become gay or queer exploring gender on the way to discovering their sexual orientation identities which are two developmental tracks but they do interface with each other…They do not tend to repudiate their bodies or feel the same kind of body dysphoria…so let’s take that same child and make that child an orange…Their explorations are typically in the realm of gender expressions rather than core gender identities. And I would say for these children nature, nurture, and culture are all strong threads.
Medical doctor Jennifer Hastings affirms the messiness of treating gender dysphoric children:
How does a medical provider say, ‘Hey, time to start cross hormones?’ So, we have guidelines and I just want to point out they are just guidelines. They’re not rules in cement or stone.
If they have concurrent mental health problems they (WPATH) state they should be addressed. Now that’s complicated sometimes…gender is sometimes is the cure. So, in order for someone’s severe anxiety and depression to go away, you can’t wait for that to go away. You need to use the cross hormone to decrease the anxiety and depression. And that’s been very problematic I think for people who read the guidelines literally…who aren’t deeply involved in this work. Because they are like, ‘Oh no no you can’t start that hormone because they ‘re not stable enough…You know this is exquisite work.
For more discussion of fruit salad (non-binary) identities and support for medical transition of minors with these identities see here.
Confidence among affirmative model advocates without solid evidentiary backing for the safety of protocols they promote
Despite the admission there are youths who are in a gray area, Ehrensaft expresses confidence around her diagnostic skills in determining who should receive medical interventions. This is a quote from ThinkProgress in an article attempting to debunk desistence from GD:
In her work, she has found that it’s not actually that difficult to glean from a child whether he simply has feminine traits or preferences or if she is insisting she is a girl. ‘If you sit down with them, you can actually sort out apples and oranges’ and distinguish transgender kids like Conner from gender nonconforming kids like Jeff.
But Ehrensaft, who also recommends medical transition for “non-binary children,” does not explain how she can predict how the permanent medical interventions she recommends for them are justified if the “gender web they weave” may “change overtime.” Can you have both the ability to make a solid diagnosis and admit that a child/teen’s identity may not be solid?
Her statements are not a substitute for studies done with control groups. And there are multiple cases of clinicians working in the field with clients, causing grievous harm with their confident assertions. The recovered memory and multiple personality disorder scandals are just a couple of examples that have occurred in more recent times.
Other PhDs are not confident in Diane Ehrensaft’s “apples, oranges, and fruit salad” diagnostics. Claudia Lament, PhD:
To be frank, I find Ehrensaft’s conceptualization of gender to be full of inconsistencies and ideology unsupported by evidence.
Kristina Olson and Lily Durwood make some arguments criticizing Debra Soh’s skepticism of child social transitions by saying:
We believe these recent articles, whose authors, to our knowledge, do not work with transgender children, overlook key differences within the spectrum of children who do not conform to gender norms, misinterpret past research, and misconstrue interventions to help transgender children.
A closer look:
whose authors, to our knowledge, do not work with transgender children
1) Other mental health and medical professionals who “worked with” clients have made horrible mistakes in the past (the recovered memory and multiple personality disorder fads the mental health community has engaged in and others involving therapist induced suggestibility). Educated mental health and medical professionals thought extreme shock therapy, lobotomies, Thalidomide, and mutilating the genitals of intersex babies were good ideas. Many other historical examples abound. There is even history of malpractice or unprofessional behavior involving gender professionals and dysphoric youth. Several cases have been covered in the news media in Britain. Her argument is an argument from authority. Experience is relevant here to the discussion but confirmation bias is also a well established dynamic in psychology and medicine. They haven’t refuted Soh’s concerns by presenting clear diagnostic criteria.
overlook key differences within the spectrum of children who do not conform to gender norms
2) Olson and Durwood have no actual hard evidence to determine which children on the “spectrum” will persist, nor if anyone in these gender clinics is actually determining this accurately, nor what the cultural effects they are inducing will have. Only a study with a control group could precisely tease out environmental effects from biological effects. It seems reasonable to argue it’s actually impossible to observe “key” differences on a “spectrum” at all. Spectrums are blurry and don’t have clear boundaries by nature, which is why so many people are very alarmed by affirmative model protocols and the potential of environmental factors to groom youth for medical transition.
These researchers may be the ones “overlooking” reality. One could just as easily say, “Olson is overlooking key similarities within the spectrum.”
misinterpret past research
3) The misinterpreting past research argument is similar to Temple et al 2018 (who attacks methodology without discrediting desistance, criticized in this piece and by Steensma. Most people who understand the data acknowledge rates of children said to be transgender may be excessively high in older studies due to a looser criterion that include youth who were just gender nonconforming. This does not mean seriously dysphoric youth do not outgrow gender dysphoria.
misconstrue interventions to help transgender children
4) They make the assumption Soh is “misconstruing” interventions, when Soh is well aware of the protocol they are advocating for and indeed worries about the psychologic impacts of it on children. What they are seem to be doing is painting Soh’s acknowledgement of developmental psychology as “misconstruing interventions” without proving her concerns wrong. This could be considered a distraction and an unwarranted assumption.
Johanna Olson-Kennedy appears confident there is no possible way hormone blockers that halt body and brain exposure to sex hormones, could have any effect on gender identity development.
Gender Odyssey, 2017:
This is a common question. People will say…’See the data shows that almost everybody who goes on blockers continues onto cross sex hormones. See were’ making ‘em trans.’ No really. That’s real, not kidding! People say that. Someone said that at Amsterdam. We don’t know why all of the kids who went on blockers went on hormones. Because they’re trans. (Audience laughs). Like there’s something really complex. Like you’re over thinking it…Could people, is it possible, is it possible, people might make a different decision?
Desist rates in studies are not zero or near zero which should at the very least raise suspicion.
Gender Odyssey, 2017:
There are people that often ask me this. If you make a suggestion to a kid about social transition you are going to make them trans (audience laughs). No, you’re not. No, you’re not! You know how I know this? For decades, we were trying to make trans people cis. And we failed miserably at that. So, it makes no sense that you can make somebody a different gender than what they are. So, I really want people to remember that. A lot of parents call me and say I don’t want to bring my kid to you because you are biased. Well I’m not going to make your kid trans if your kid isn’t trans.
Historical evidence of trans adults is not scientific confirmation that all children and teens who experience gender dysphoria will have immutable cross-sex identification completely unaffected by environment. There is evidence to the contrary.
Ray Blanchard is a psychologist and expert on gender dysphoria in adults. Here he questions themes related to what he sees as self-confidence in Ehrensaft, K. Olson, J. Olson-Kennedy, and others.
Some of them will flatly say that they can tell. They know. They can clinically differentiate on the basis of interviewing patients, which ones are truly transsexual and which are just, what should we call them, “faux transsexual.” This must make them great clinical geniuses because none of the real-life clinicians I know, get diagnosis right 100% of the cases, or predict prognosis in 100% of the cases correctly. So, I guess the field of affirmative therapy is lucky to have these Olympian figures who look right into the soul of a kid and differentiate those who are the real article from those who are at risk of desisting. And having made a horrible mistake in their lives.
Problems with the Trans Youth Project study and NIH study
In addition to what might be problems with Kristina Olson’s arguments there are other possible problems with the way she describes her study and its goals. The goals are summarized below.
The TransYouth Project is only the first part of Olson’s grand vision for new research on the gender of kids. As recruitment comes to a close for kids who have socially transitioned, she and her colleagues are also recruiting a whole separate cohort of kids who are gender nonconforming but who have not socially transitioned — i.e., a group that more closely resembles the participants in the desistance studies. By intentionally distinguishing this group from the trans kids and then following them into adulthood, Olson will be better equipped to draw the kinds of predictive conclusions the desistance studies tried to draw about who will grow up to be trans and who won’t. “[W]e expect at least some of them will socially transition, so that will give us some data from before and after,” she explained. But for those who do not identify as trans, “we’ll also be able to see if there are patterns of response in early childhood that predict who ends up socially transitioning or who identifies as trans later in life based on their presentation when they were very young.
… she and her colleagues are also recruiting a whole separate cohort of kids who are gender nonconforming but who have not socially transitioned.
This, in reality, is not effective in determining the effects of early social transitions and early Lupron use on children diagnosed with gender dysphoria or desistance rates, which are the two most important questions that need to be answered. Unless they have another cohort, whose children are loved and supported in their gender nonconformity but raised in a body acceptance / transition as last resort model, the study won’t answer the main questions people need answered. The study cannot address long-term safety without a cohort to compare who have the same level of gender dysphoria raised in different circumstances. Comparing socially transitioned children to other gender nonconforming children is irrelevant.
At follow up after social transitions, she has shown that her cohort has mental health rates comparable to controls (Olson 2016). It is good that these children are not experiencing high rates of distress as is the case in most other studies. But its notable many other studies show high rates of comorbid mental health conditions and that the youth come from trans-tolerant countries, often with supportive parents who brought their children to clinics for help (Canada, England, Sweden). Olson admits these may be particularly mentally healthy families. In addition, her sample is of volunteers and is not representative.
Olson omits that it is expected that a social transition would make a dysphoric child temporarily happier. The child doesn’t have any concept of the consequences of hormone blockers, the potential for destroyed sexual function, the reality of honeymoon transition periods, the consequences of invasive surgeries, or the fact that most people (particularly heterosexual men) will want partners of the opposite biological sex. A snapshot result of social transition is not a complete picture of gender identity or long-term outcomes or if an easier childhood is worth a lifetime of medical consequences. It seems these would be relevant points. Yet, in this article, parents are just told how to raise “happy and healthy” trans kids. They do not mention gay and lesbian people once.
There may be issues with another study funded by the NIH, which supports the most ardent affirmative model advocates such as Johanna Olson Kennedy and Norman Spack.
An article called “What’s Wrong with the New NIH Study on Transgender Kids?” from a more conservative website offers reasonable criticisms:
Unfortunately, multiple aspects of this study indicate that it is intended to produce evidence supporting a particular conclusion: that transgender affirmation therapy is safe and effective for gender-dysphoric youngsters. And once the federal government speaks, states and other institutions will fall in line.
The Child and Adolescent Gender Center Clinic at UCSF Benioff Children’s Hospital San Francisco, directed by Dr. Stephen Rosenthal, describes itself as offering “the mental health, medical, advocacy and legal expertise necessary to support a healthy transition.” Dr. Johanna Olson of Children’s Hospital Los Angeles opines that “[transgender] young people can really benefit from not going through the wrong [sic] puberty the first time.” Dr. Norman Spack of Boston Children’s Hospital describes treatment that harmonizes the psyche with the biological sex as “noxious.” And in his practice, Dr. Rob Garofalo of Lurie Children’s Hospital in Chicago employs irreversible cross-sex hormone treatment with children as young as fourteen, even though he admits he doesn’t understand the long-term consequences.
All four of these researchers, then, are deeply invested in affirmation therapy. The chances their study will find serious harm from these interventions are pretty slim.
The design of the study is similarly problematic. As described by UCSF, the study will include 280 youth from two age groups: younger children in early puberty, who will be administered puberty-blockers, and older adolescents, who will be given cross-sex hormones. Then the researchers will see how these protocols work out.
Notice any group missing from this lineup? A control group. Except in certain very limited circumstances, medical research studies are usually “randomized controlled studies,” which include a control group of study participants who don’t receive the therapies being evaluated. Comparing outcomes between a group that receives the therapies and one that doesn’t is the “gold standard” of research, in accordance with the Good Clinical Practices and Human Subject Protections required by the Food and Drug Administration for pharmacological studies.
Another troubling design feature of the study is the time frame. The children will be studied for only five years. Presumably, if eleven-year-olds receive puberty blockers, are still generally satisfied with the treatment at age sixteen, and at that point show no adverse medical effects, the researchers will declare the therapy a success and recommend this treatment for transgender children.
Pediatric endocrinologist Van Meter considers this one of the worst features of the study. He maintains that children’s satisfaction with their “new sex” a few years after the therapy begins is essentially meaningless, especially when the study is designed to place the children and their families in a safe bubble in which their transgender identity is affirmed. The rubber will hit the road, Van Meter predicts, ten, twenty, or thirty years later, when the children become adults and realize they must live the rest of their lives struggling to fit into a society that will not reshape itself to accommodate their situation. And they must do this with infertility and potentially even life-threatening medical conditions resulting from the hormone treatments and, if they go on to have sex-reassignment surgery, with mutilated bodies.
By stopping the study of dysphoric youth at five years, when many of the participants will still be in their teens and the rest in the earliest stages of adulthood, the NIH researchers can mask these tragic consequences that may appear later. The study will thus be able to trumpet the success of affirmation therapies and reassure doctors that they should adopt these practices. Subsequent research will cite these conclusions to build a body of “evidence” that will shape federal and state policies regarding treatment of individuals with gender dysphoria.
Gender dysphoria as a “normal variation” in human beings
One argument that appears politically motivated rather than logically or scientifically informed is that transsexualism is a “normal variation” of human behavior. This argument is ubiquitous in pro-medical transition resources regarding youth with gender dysphoria (sites labeled “LGBT,” gender therapists, and gender clinic websites).
Below is one of many examples:
An alternative view is that a transgender identity is a normal variant of human gender identity, and that trans- gender children are expressing their “true” identities. Under this view, the therapist’s role is to support and affirm their identities.
No one deserves to be stigmatized, regardless of their quirks, mental health issues, or harmless kinks. Shaming is harmful to people. But this is an emotionally and politically strategic argument, not a rational one. Gender-atypical people have indeed existed throughout history. But the idea promoted by trans activists that surgeries and cross-sex hormones are “medically necessary” to avoid an individual experiencing poor mental health or suicide doesn’t make this condition a “normal variation,” any more than schizophrenia or Down syndrome are “normal variations.” Animals, including primates, also display gender atypical behavior but are not pulling off their genitals to exist in the world. This argument appears to be designed to acclimate parents, public schools, and insurance companies to the idea that giving children hormone blockers is normal and healthy.
In a petition regarding a much criticized policy statement by the American Academy of Pediatrics (AAP), the writers sum up the problems with this argument:
(1) The problem of diagnosis
Rafferty et al. state “transgender identities and diverse gender expressions do not constitute a mental disorder.” (p 4) and “Some youth who identify as TGD also experience gender dysphoria, …” (p 3)If transgender-identification is not a mental disorder, what is it? Is it a medical condition? If so, how is it diagnosed? How can the TGD “condition” be both a mental health disorder for “some youth” and not for others but both are treated the same way?
These questions are never answered directly by Rafferty et al. or other “trans experts,” as well as the American Psychological Association (APA) and the World Professional Association for Transgender Health (WPATH) because the answer is simply that the youth just needs to proclaim that they are transgender – it is purely self-diagnosed. If “being transgender or gender diverse” isn’t a mental disorder or a medical condition, why are youth treated with the life-altering, non-FDA-approved drugs (experimental GnRH agonists are used for years and hormone therapies are used for a lifetime) and irreversible, serial cosmetic surgeries in an attempt to achieve a scientifically impossible goal?
We have experienced doctors giving prescriptions without adequate mental health consideration and after only 1-2 visits.
Summary: Diagnosis is the youth’s self-diagnosis. The life-altering medical treatments offered do not match the diagnostic process or the clinical evaluation standards of medicinal or surgical safety and efficacy.
An observation about the uniqueness of gender dysphoria as a mental condition and it’s medical treatment below:
This claim is important, for if trans were a disorder (as in 1966), the work of the clinic would belong in a worrying tradition, one that harks back at the worst to lobotomy and calls up disturbing memories of the treatment of David Reimer. If trans has any links to body dysmorphia, to anorexia, or to self-harm, then it could not be appropriate to medicate or to offer surgery, however acceptable to the patient, however fiercely demanded. Colin Ross identifies the underlying ethical problem:
Gender identity disorder is unique among all DSM-IV-TR diagnoses. It is the only disorder in which treatment is designed to confirm, reinforce, and validate the belief that is the basis of the mental disorder. In all other diagnoses, the symptoms in the diagnostic criteria are viewed as pathological and the goal of treatment is to remove the symptoms. In gender identity disorder, however, the body is altered to match the belief that is said to be a symptom of mental disorder. This is self-contradictory. Either gender identity disorder should be dropped from DSM-V, just as homosexuality was dropped from the diagnostic system, or gender reassignment should be discontinued. The core contradiction in the current approach to gender identity is an ethical problem in the mental health field.[22] –Lisa Marchiano
H. Miscellaneous comments
Below are just some interesting, random quotes.
On Dr. Spack’s enthusiasm for hormone blockers:
When he learned about Dutch doctors who were using puberty blockers on patients, “I was salivating,” Dr. Spack told the New York Times last June (emphasis mine). “I said we had to do this.”
Dr. Spack compares trans girls to Russian dolls and talks about how hormone blockers to cross-sex hormones make them look “normal” and “beautiful.”
This comment calls into question the ethics of valuing normalcy and beauty to pass better and be sexually arousing to heterosexual men over not sterilizing a child, not destroying sexual function and choice about bottom surgery, not affecting cognitive function, and not causing possible long-term health consequences.
Dr. Olson-Kennedy seems to embrace trans activism:
Gender Odyssey, 2017:
The parent desperately wants you as the professional to close that gap and by pushing their kid backwards. But you as a professional know that you have to close that gap by pushing the parents forward.
And:
We are not only providers. We are advocates. And we have to own our advocacy.
What appears to be Olson’s anti-gatekeeping attitude:
If you see gender-dysphoric 13- and 14-year-olds not as young people with a condition that may or may not indicate a permanent identity, but as trans kids, full stop, it makes sense to want to grant them access to transition resources as quickly as possible. Olson-Kennedy said that the majority of the patients she sees do need that access. She said she sees a small number of patients who desist or later regret transitioning; those patients, in her opinion, shouldn’t dictate the care of others.
Olson-Kennedy finds articles about child masturbation interesting but may be permanently destroying sexual function in her minor patients:

Affirmation model advocates seem to present sterilizing minors as not that important, which is interesting because doctors often refuse grown women who have already had children sterilizing procedures due to ethics concerns. A Medium post draws attention to Jack Turban’s intentional downplaying of the reality of sterilization with trans-medical affirming protocols implemented on children:
A Psychology Today article supposedly ‘debunking junk science’ (of the American College of Pediatricians, which produces anti-gay material), starts with the well-known facts that reparative therapy is a bad idea, and that gay parents are fine, and then promotes actual junk science by promoting ‘affirming transgender youth’. It also manages to lie about the fact that transgender children are, in fact, sterilized by their treatment.
Kelly Winters (an active WPATH member) and Dianne Ehrensaft seem to observe almost mythical wisdom in trans children around their views on raising children, as if tweens and teens have a proper understanding of this:
4thwavenow reviews Diane Ehrensaft promoting a similar narrative around permanently sterilized minors:
And that’s not all: Ehrensaft goes on to shame these recalcitrant parents with the implication that puberty-blocked, 11-year-old trans tweens are more socially responsible than their clueless parents:
“And what I will say about many of the youth who want puberty blockers is: I have never met such an altruistic group of kids around adoption! Never! “I will adopt because there are so many children who need good homes.” And I think that’s both heartfelt but also they’re trying to tell us the most important thing to me right now is being able to have every opportunity to have my gender affirmation be as complete as possible. Anything else is secondary.”
Do we need a PhD in developmental psychology to tell us this? You bet an 11-year-old thinks anything but what they want RIGHT NOW is secondary. I want it, and I want it right now: the motto of youth, of children who are a decade or more away from full development of their reasoning, judgment, and awareness of future consequences.
I. Promote the idea that parents only have two options: The transition or suicide narrative that suggests either allow medical transition for their child or teen or they will kill themselves
Both trans-identified teens and adults have a higher risk for suicide. This should not be taken lightly. We do not advocate for any rejection of trans-identified minors or for them to receive a message that they will be less valued by their parents if they transition. Family rejection correlates with much poorer mental health for transgender people. But whether or not that should translate into unquestioning social and medical affirmation of minors is debatable. But that is not how affirmation model advocates promote this discussion. Many give parents and the public the message that you should adopt the affirmation model or be ready to have a dead child. Some of the most prominent professionals are doing this (Ehrensaft and Olson-Kennedy), and it is creating a cultural environment that is contrary to the way organizations such as the American Foundation for the Prevention of Suicide and other suicide prevention organizations recommend discussing suicide and how to stop it. Suicidality in trans youth and adults is a complicated topic. Transition may reduce suicide risk, but not all studies confirm this. For an in-depth discussion of research on transition and its effects on mental health and suicide risk, see this section.
J. Financial gain & off label use of drugs
We expect doctors and therapists to be involved in discussions about drugs used in their areas of expertise. One in-depth article in Medium about funding for transgender advocacy and medical care alleges that there may issues with promoting protocols tied to financial gains. We can’t make any claims about its validity. However, generally, transition creates profits for some individuals, including doctors and drug companies:
Follow The Money
Let’s look at three doctors in particular. Their names are Dr. Diane Ehrensaft, Stephen Rosenthal, and Johanna Olson-Kennedy. Why?
All three of those names have had a financial relationship with AbbVie, maker of Androgel and Lupron, amongst other hormone replacement therapies and GnRH agonists. All three have gone on to promote the off-label use of AbbVie products to treat transgenderism. Both Joanna Olson and Diane Ehrensaft attended an AbbVie advisory board on gender care, Olson in 2015 and Ehrensaft in 2014. Olson discloses this as a conflict of interest in the paper Care of a Transgender Adolescent Commentary, which was published July 2015 — she attended this advisory board after submission and was compensated for attending. Olson then continued promoting off-label use of AbbVie drugs. Diane Ehrensaft does not declare this as a conflict of interest on any research papers, but it appears in her Curriculum Vitae (scroll to page 16), which she submitted to court while an expert witness, and is hosted on her website. Her CV reports, that in 2014, she was a board member of the ‘AbbVie Trans Advisory Board’, while promoting their drugs for off-label use in transgenderism, both in academia and through popular science books she wrote, such as The Gender Creative Child. Was she compensated for being on this advisory board, like Olson? Stephen Rosenthal frequently discloses that he is a consultant for AbbVie as a conflict of interest in both interviews and research, and then continues to promote the dangerous off-label use of their medication in adolescents.
Why is this concerning? The Center for Medicaid and Medicare Services advises that among the methods of spotting unlawful, off-label promotion, is paying physicians to serve as advisory board members.
Another quote:
Stephen Rosenthal is a consultant for AbbVie while giving lectures and media interviews essentially promoting the use of AbbVie products in ‘transgender children’. I would say that none of this passes the smell test at all. If there isn’t an inappropriate relationship between these scientists and AbbVie, they need to come clean on what exactly is going on between them and the company. Ehrensaft has not disclosed this as potential conflict of interest at all in either research or in media interviews. Given that she is promoting the use of AbbVie drugs in popular media through her own books that is extremely concerning. These scientists go out and promote the use of these drugs for transgenderism in popular media, arguing that it should be a civil right. They and others disseminate misleading information about transgenderism to the media. Rosenthal and Olson, along with Garofalo and Spack are leading a long-term observational study of transgender children going on puberty blockers and cross-sex hormones. How can they be neutral on this when both have a financial relationship with AbbVie? How can we be sure that this study — or any other studies by theses scientists or even with collaborators is not biased because of this relationship? What about the long-term studies they are involved with? Is the result of those studies already pre-determined, because of the financial fortunes to be made?
Also:
Other scientists are also possibly monetarily compromised beyond redemption. Robert Garofalo, who is a co-author of many of the recent studies on transgenderism, particularly in children, works for Lurie’s Children’s Hospital, where the Gender and Sex Development program he directs was started with seed money from Jennifer Pritzker, and continues to receive donations from the billionaire. How does this affect his research and opinions? If he disagrees with Pritzker, who is ideologically motivated towards a certain conclusion, he will no longer be employed at a prestigious children’s hospital. It is far too large a conflict of interest, and it is not declared in his research. How can any of it possibly be impartial? What is even more worrying, is that they lie to the media, and that the media does not question their narrative.
Another quote from The Federalist:
Moving from ideology to good old-fashioned self-interest, it’s worth noting that the Olson-Kennedy team apparently benefits financially from their “affirming” treatment beyond just insurance reimbursement for services rendered. Both are on the consultant payroll (website censored by Wordpress) for Endo Pharmaceuticals, which formulates and markets the hormones administered to dysphoric patients (administered frequently off-label, which means the hormones haven’t been approved for this purpose). If this team were in any other line of medicine, activists would be screaming about the conflict of interest.
Transgendertrend, a site questioning the rise of children being diagnosed as transgender, makes this observation:
I would want to know why a drug company, Ferring, sponsored the crucial Dutch trial into puberty blockers: the 2006 Delemarre-van de Waal and Cohen-Kettenis paper was ‘presented at the 4th Ferring Pharmaceuticals International Paediatric Endocrinology Symposium, Paris (2006)’ and Ferring Pharmaceuticals supported the publication of these proceedings.’
Ferring was interested in this novel use for their expensive drug because they market Triptorelin, one of the GnRH antagonists used in gender clinics under the brand names Diphereline and Gonapeptyl.
The Amsterdam clinic was financially supported in its experimental project to block puberty in gender dysphoric adolescents by a pharmaceutical company which stood to make commercial gains from their new protocol.
© Gender Health Query, 6/1/2019
References for Topic 4
Updates Topic 4
CONTINUE TO TOPIC 5:
MENTAL HEALTH & MEDICAL PROFESSIONALS HAVE MOVED FROM A MENTAL HEALTH SCREENING MODEL TO A GENDER DYSPHORIA AFFIRMATIVE MODEL
Contents
4) Comments safety / desistance unknown
A. Socially & medically experimenting on patients
B. Adult influence on trans identification in minors?
C. Unsubstantiated claims social transitions are “fully reversible”
-Multiple statements on the “reversibility” of an early gender social transition
-Evidence social transitions may in fact increase persistence
-Not all gender professionals support early social transition
D. Unsubstantiated claims hormone blockers are fully reversible
-Multiple statements on the “reversibility” of hormone blockers
-Hormone blockers may effect the gender identity of the youth & increases persistence
-Methodological flaws arguments don’t prove desistance numbers are statistically irrelevant
-Framing discussions of desistance as transphobic may risk desisting children
-Gender dysphoria experts who acknowledge desistance
F. Obscuring the link between gender dysphoria & LGB adults
-Gender dysphoria & its connection to adult LGB identity
-Affirmative model avoids discussion of the connection between adult homosexuality & childhood GD
-Desisters were really closeted trans people
G. Statements demonstrating lack of clear diagnostic criteria
-Apples, oranges, & fruit salad
-Confidence among affirmative model advocates without solid evidentiary backing
-Problems with The Trans Youth Project Study & NIH study
-Gender dysphoria as a “normal variation” in human beings
I. Promote the idea that parents only have 2 options, transition or suicide
J. Alleged possible conflicts of interest due do financial gain
BACK TO OUTLINE
More
1. Do Children Outgrow Gender Dysphoria?
3. Are children & teens old enough to give consent?
4. Comments safety / desistance unknown
5. Gender dysphoria affirmative model
6. Minors transitioned without any psychological assessments
8. Regret rates & long term mental health
11. Why are so many females coming out as trans / nonbinary?
13. Why is gender ideology being prioritized in educational settings?
14. Problems with a politicized climate (censorship, etc)