

TOPICS
For those new to this issue it’s best to know these terms before reading.
1) Do children and teens with serious gender dysphoria ever outgrow gender dysphoria? Yes
Desistance/persistence are the terms for youth who do and do not outgrow gender dysphoria. These two cohorts usually separate in puberty. Despite a lack of reporting on this issue in the media, and factually incorrect information often presented by trans activists (as well as some pro-affirmation model professionals and journalists), some seriously dysphoric minors desist. All studies on gender dysphoric youth confirm desistance (reviewed below).
Studies also consistently show an association between childhood GD and homosexuality in adulthood and sometimes bisexuality (reviewed below). In earlier studies, children with childhood-onset dysphoria and who remain dysphoric into their teenage years are said to be likely to be trans-idenitified in adulthood by some gender clinicians. In the past, many desisted after experiencing some puberty.
We seek to learn what will happen to children socially transitioned as young as 4 years old and prescribed hormone blockers at increasingly younger ages (9-11 years old in some cases). In addition, we seek to learn what will happen to unprecedented numbers of teenage females and young adults identifying as trans or non-binary after puberty starts. This is a previously unstudied dynamic among gender clinicians.
While social transition may temporarily reduce depression in children with GD, according to one study, there is no evidence that social transition is benign for children who may outgrow their distress. It’s unknown if positive reinforcement of children’s gender dysphoria affects their gender identity outcomes. Researchers have not done studies with control groups. In the current climate, it is considered unethical not to affirm a child’s transgender identity. However, we don’t know how affirmation will affect children who might otherwise naturally desist.
Desistance rates from prior studies (sometimes found to be as high as 80%-90%) are most likely inflated because minors may have fallen under a diagnosis that’s less stringent than the current DSM-V. This is relevant because there is an intense effort to focus criticism on the methodology of prior studies to discredit desistance altogether.
However, it is inaccurate to say that all truly dysphoric children and teens grow up to be transgender adults. And the impact of the gender-affirmative model protocols on those who would not ultimately identify as trans if allowed to mature should not be considered irrelevant. There is an attempt to characterize desisters as merely “boys who liked pink,” but children diagnosed under previous DSM IV criteria often had clinical distress.
Disclaimer: In the past, some mental health professionals employed behavior modifications to reduce cross-sex behavior in the hopes of increasing desistance. We do not endorse this practice and fully support a youth’s right to express themselves contrary to gender stereotypes. We are concerned that reinforcing a “born in the wrong body” narrative in gender-nonconforming children will likely prime a minor for a medicalized path. We endorse body-positive mental health support and time for maturation.
Many LGB and trans-identified people, mental health professionals, doctors, and parents believe subjecting minors to unnecessary experimental medical procedures is unethical. For a breakdown of these arguments, see Moral Dilemmas.
A. Changes to DSM-V childhood & adolescent gender dysphoria
In the "Diagnostic and Statistical Manual of Mental Disorders" (DSM-V, implemented in 2013), used by the mental health profession, some criteria are slightly different from the DSM criteria used in earlier research. However, the similarities outweigh the differences. The most significant difference between DSM-V, DSM-III and DSM-IV (used since 1994) is that "gender identity disorder" was changed to "gender dysphoria." They did this to destigmatize the condition and paint the distress as the problem (rather than portray the desire to be the opposite sex as the problem). This way, it's not a disorder in their minds if a child is no longer distressed after a social transition. And wanting medical interventions is just a healthy part of "gender diversity." Identity politics were behind the push for this change:
For years advocates have lobbied the American Psychiatric Association to change or remove categories labeling transgender people in a psychiatric manual, arguing that terms like “Gender Identity Disorder” characterize all trans people as mentally ill. Based on the standards to be set by the DSM-V, individuals will be diagnosed with Gender Dysphoria for displaying “a marked incongruence between one’s experienced/expressed gender and assigned gender.
Another motivation for these changes is to move towards an informed consent medical model rather than a mental health model. The most critical differences between DSM-IV and DSM-V relevant to desistance stats are summarized below. A full review can be found here:

The criteria for childhood and adolescent DSM-V gender dysphoria is listed below. The-6 month criteria will be relevant to discussions later around the high rates of female teenagers identifying as trans. While some youth satisfy the criteria for GD for a year or more (longer than the required 6-month period for an official DSM diagnosis), there are many who outgrow the strong desire to transition. Undertaking medical interventions puts them at risk for the permanent effects of testosterone and breast amputation which is being performed on tween and teenage females.
“Consistent, insistent, and persistent” is a common query to test for a “true trans” child or teen:


Below is a list of criteria for childhood GD under a DSM-IV diagnosis. It’s relevant to note that distress was an important factor, even under the old definition. This is pertinent because the often-used argument is that children diagnosed before the less stringent DSM-V were just gender nonconforming children. However, data and clinical observations show that some distressed children with an official DSM diagnosis will ultimately outgrow GD (see below for details). It’s not accurate to claim that desisters diagnosed under DSM-IV or earlier would not have met the criteria under DSM-V.
DSM-IV criteria for childhood gender identity disorder:
A. A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex). In children, the disturbance is manifested by four (or more) of the following:
(1) repeatedly stated desire to be, or insistence that he or she is, the other sex
(2) in boys, preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
(3) strong and persistent preferences for cross-sex roles in make-believe play or persistent fantasies of being the other sex
(4) intense desire to participate in the stereotypical games and pastimes of the other sex
(5) strong preference for playmates of the other sex. In adolescents and adults, the disturbance is manifested by symptoms such as a stated desire to be the other sex, frequent passing as the other sex, desire to live or be treated as the other sex, or the conviction that he or she has the typical feelings and reactions of the other sex.
B. Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex. In children, the disturbance is manifested by any of the following: in boys, assertion that his penis or testes are disgusting or will disappear or assertion that it would be better not to have a penis, or aversion toward rough-and-tumble play and rejection of male stereotypical toys, games, and activities; in girls, rejection of urinating in a sitting position, assertion that she has or will grow a penis, or assertion that she does not want to grow breasts or menstruate, or marked aversion toward normative feminine clothing. In adolescents and adults, the disturbance is manifested by symptoms such as preoccupation with getting rid of primary and secondary sex characteristics (e.g., request for hormones, surgery, or other procedures to physically alter sexual characteristics to simulate the other sex) or belief that he or she was born the wrong sex.C. The disturbance is not concurrent with a physical intersex condition.
D. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
The most relevant criterion, is section D: “The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.” As D was necessary for a GID diagnosis, even under the older definitions, children who were simply gender nonconforming, technically, should not have been diagnosed with GID. Their dysphoria had to be serious enough to cause “distress or impairment.”
In addition, criterion B includes hatred of one’s own genitalia. This is pertinent because the argument is often used that children diagnosed before DSM-V were really just gender nonconforming children who did not conform to gender expectations. A review of research, observations of serious cases by mental health professionals, and the “distress” which was required under DSM-IV, indicates it’s unlikely that so few of these children would be considered clinical today, as to not warrant any concern for their well-being (under a dysphoria affirmation model).
B. Desistance/persistence statistics & the association with childhood GD & adult LGB identity
Studies on youth and gender dysphoria show that some children outgrow dysphoria and are statistically much more likely to be LGB than the general population. An interesting longitudinal study in Britain confirmed a strong correlation between homosexuality and early cross-sex behavior (see graphs for boys and girls below):


The Avon Longitudinal Study of Parents and Children (ALSPAC), also known as Children of the 90s, is a world-leading birth cohort study, charting the health of 14,500 families in the Bristol area. Graphs created from Li’s data with permission by Oxford’s Michael Biggs here
The Avon Longitudinal Study of Parents and Children (ALSPAC), also known as Children of the 90s, is a world-leading birth cohort study, charting the health of 14,500 families in the Bristol area. Graphs created from Li’s data with permission by Oxford’s Michael Biggs here
James Cantor, a PhD clinical psychologist and sexologist, summarizes the data on dysphoric minors and desistance rates in a blog post called “Do trans kids stay trans when they grow up.” He finds that a high percentage of youth grew up to be LGB, not trans, when studies looked at sexual orientation:

James Cantor, Sexology Today desistance stats, “Do trans- kids stay trans- when they grow up?”
This article reviews what the collective data says on sexual orientation and desistance. Note that same-sex attraction in females may be underrepresented in this review, as it is very common for bisexual and lesbian females to “come out” in their twenties, much later than their heterosexual and gay peers:
The percentage of desisters with same-sex attractions (by fantasy):
Bakwin to Kosky – 41.7%
Green – 74.4%
Zucker & Bradley – 24.2%
Wallien & Cohen-Kettenis – 50%
Drummond – 28.6%
Singh – 56.5%
Steensma – 48.8%
The below graphic is from the full findings which can be found here:

Paul Dirks, “Desistance Master Chart”
“Gender Identity Disorders in Childhood and Adolescence” (Korte et al., 2008), discusses the high rates of gender dysphoric children who are potentially same-sex attracted youth:
Experience has shown that, in not a few cases, a strongly and resolutely asserted desire to change to the opposite sex becomes markedly neutralized over the course of time, and the individual later undergoes a homosexual "coming-out" (1, 3). In view of this fact, it must be understood that early hormone therapy may interfere with the patient's development as a homosexual. This may not be in the interest of patients who, as a result of hormone therapy, can no longer have the decisive experiences that enable them to establish a homosexual identity.
Here, Polly Carmichael, the Director of Tavistock’s youth gender services, states:
The available evidence suggests that most prepubescent children with gender dysphoria will have a different outcome in adulthood, Carmichael says: “The most common would be one around sexuality, rather than gender identity.” In her experience, they are more likely to be LGB than T
It appears there are efforts among some gender-affirmative model advocates to avoid or suppress discussion of the correlation between childhood GD and homosexuality to promote the “innate gender” identity narrative that supports early childhood social transitions.
Desistance stats breakdown of DSM positive children (more severe dysphoria beyond gender nonconformity)
Because some parents bring their gender nonconforming children to professionals, even when the children are not dysphoric, it is helpful to narrow down desistance data in more recent studies where youths were diagnosed primarily under DSM- IV. As previously explained, DSM-V diagnostic criteria are slightly more stringent, although distress was still a feature of previous DSMs.
Here is a list of the more recent studies containing desistance information.
Drummond et al (2008)
Wallien and Cohen-Kettenis (2008)
Singh (2012)
Steensma et al (2013)
Dr. Kenneth Zucker is one of the world’s most experienced psychologists specializing in youth gender dysphoria. He was the head of CAMH’s Family Gender Identity Clinic for over 30 years before they fired him as the result of an activist campaign against him. He has since been exonerated and awarded a large settlement. While he helped some of his young patients transition, he also advocates for a cautious approach (and is, therefore, a target for trans activists who believe this caution amounts to conversion therapy. In a blatant show of disregard for Dr. Zucker’s expertise at the inaugural 2017 USPATH conference, Zucker’s mini-symposium was disrupted and his 2nd panel was canceled after activists protested.
The graphic below shows the results (averaged from the above studies) from Dr. Zucker’s review of the desistance rates for gender dysphoric minors. What makes Dr. Zucker’s presentation so useful is he isolated the data of youth with a DSM diagnosis (so the ones represented in the data below are only dysphoric youths and not merely gender nonconforming youth):
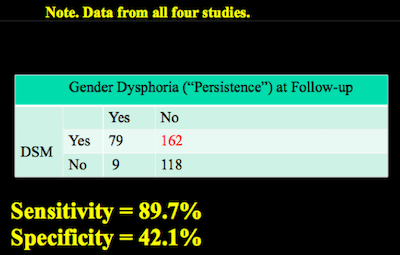
Zucker, Power Point presentation USPATH 2017
The relevant point here is that out of 241 children with a DSM diagnosis, 162 desisted. That is, 67% of all children with dysphoria serious enough for a DSM diagnosis. However, 7% of youth who end up in the persistence category were not diagnosed under DSM criteria. There is no black and white way to screen for who will desist/persist:

Zucker, Power Point presentation USPATH 2017

Affirmation model advocates, such as Diane Ehrensaft (2018) and Kristina Olson (2015), indicate they believe trans-idenitifed children who say they are the opposite sex in childhood are, in fact, "trans," as they appear to be just like natal girls and boys in behavior and interests. Other mental health and medical professionals dispute that this is known to be true all of the time and are thus worried about the effects of early social transition for these children.
The graphic below is from Dr. Zucker's canceled symposium at USPATH. It highlights that the "I am" claim is not a clean diagnostic screening tool:

Zucker, Power Point presentation USPATH 2017
There are efforts to discredit or downplay desistance data based on the methodology used in the various studies. While few studies are perfect, the contentious studies had opportunities to track this relevant information. Desistance deniers are never able to discredit desistance altogether. Korte et al. (2008), reiterates the reality of desisters even among those who have severe dysphoria:
Even among children who manifest a major degree of discomfort with their own sex, including an aversion to their own genitalia (GID in the strict sense), only a minority go on to an irreversible development of transsexualism (6). Irreversibility of the manifestations, however, is considered to be an indispensable requirement before the diagnosis of transsexualism can be made, or any body-altering treatments initiated.
New information on desistance in tween, teen, & young adult onset gender dysphoria (ROGD) occurring mostly in females
Given the recent rise in young females coming out as transgender —even after not having experienced gender dysphoria as a child, or gender nonconformity—a researcher at Mount Sinai, Lisa Littman (now at Brown University), decided to study some possible reasons for this new phenomenon:

As we know, many youths who experienced GD in childhood were likely to desist as they went through puberty. The ones who did not would then transition (as their identity was unlikely to change at that point).
It is significant to the discussion about the rapid rise in tween and teen females who come out as trans, that in all previous studies, GD was present in childhood, which is not the case for many of the youth described in Littman’s study.
It is possible that many in this new, growing group of young females have less stable trans identities than the gender dysphoric children who remain trans-identified into their later teenage years. Those who only come to identify as trans in their teen years are more likely to desist even after meeting the 6-month DSM minimum used to justify medical transition of minors. More may desist as they grow older:
This section reports on the duration of AYA transgender-identification (time from the AYA’s announcement of a transgender identity until the time the parent completed the survey) that covers, on average, 15.0 months (range 0.1–120 months) with a median of 11 months (Table 12). The steps taken towards transition during this timeframe are listed in Table 12. At the end of the timeframe, 83.2% of the AYAs were still transgender-identified,5.5% were not still transgender-identified (desisted), 2.7% seemed to be backing away from transgender-identification,and 8.6% of the parents did not know if their child was still identifying as transgender. Descriptions of backing away or moving from transgender-identified to not transgender-identified include the following. One parent observed, “She identified as trans for six months … Now back at school, she is thinking maybe she's not trans.” Another parent offered,“My daughter [identified] as trans from ages 13–16. She gradually desisted as she developed more insight into who she is.”One parent described that after one year of identifying as transgender, “basically, she changed her mind once she stopped spending time with that particular group of friends.” The duration of transgender-identification of the AYAs who were still transgender-identified at the time of survey was compared to the duration of those who were no longer transgender-identified and those who seemed to be backing away from a transgender-identification (combined) by t-test. The difference between these groups was statistically significant (p = .025), with a t-value of -2.25 showing that those who were no longer transgender-identified and backing away had a longer duration of identification (mean = 24.1 months) and those who were still transgender-identified had a shorter mean duration (mean = 14.4 months).
The study’s findings on duration of transgender-identification suggests that a longer observation period might reveal greater rates of desistence and is consistent with anecdotal reports of adolescents who desisted from rapid-onset gender dysphoria approximately 9 to 36 months after presentation.
Will living full-time as the opposite sex & early hormone blocker use increase persistence?
How a gender social transition affects children is one of the most critical questions that health professionals must answer. Yet few appear to have an interest in determining this. In addition, information around this issue is actively censored by USPATH/WPATH, the organization most influential in disseminating information about trans youth health care.
In addition, the gender-affirmative model is employed without data to prove it has no (negative) effect on the psychosexual development and gender identity of would-be desisters who were previously more likely to grow up LGB (or perhaps heterosexual) than transgender.
One study in fact shows a correlation between early social transition and persistence (Steensma et al., 2013), which is interpreted in two ways:
There are two interpretations of this information.
1) Since persistence is associated with the severity of gender dysphoria, it may be that social transitions only occurred in severe cases (and that social transition may provide the best mental health support for “truly trans” children).
2) While 1 may be true for an unknown percentage of trans-identified youth, social transition also tracks would-be desisters for gender reassignment by denying them the opportunity to mature into accepting their biological sex (thereby avoiding a medical-dependent identity, which would be an unethical outcome for those particular children).
Psychologists Diane Ehrensaft and Kristina Olson, Dr. Michelle Forcier MD, MPH, and endocrinologists Dr. Johanna Olson-Kennedy and Dr. Norman Spack are some of the lead proponents for socially transitioning young children. Therapists, “LGBT” organizations, and school education programs are rapidly embracing this model. Social transition is now the norm, not the exception, and parents report great difficulty finding therapists who do not immediately affirm a child or teen as trans.
Not all mental health and medical professionals agree it is safe for all dysphoric children to transition socially. Some are concerned that the affirmative model channels youth who, if otherwise left alone, would naturally outgrow gender dysphoria. Those who socially transition may not receive needed support for coping with GD in other non-medical ways.
Dr. Kenneth Zucker is one of those who is concerned. Zucker’s critics claim that some of his techniques involved behavior modifications to help a child adjust to their natal sex. These strategies are not supported by Gender Health Query or by many skeptics of child transitions. However, what liberal and “LGBT” media reports never mention is that Zucker was cautious in his approach to protect gay youth (and other GNC youth) from over-medicalization. He believes what he calls a “GST” (gender social transition) will prevent the natural desistance process in youth that are (according to statistics) more likely to be LGB, not trans-identified:
I predict, therefore, that in contemporary cohorts of children who experience a GST prior to puberty that the rate of GD persistence will be substantially higher than that reported in the follow-up studies to date
A presentation by the psychologists from the leading gender dysphoria treatment clinic in Britain, posted on the WPATH website, indicates more cause for concern. There is a very high association between social transition and later treatment with hormone blockers leading to persistence rates that seems to be much higher than before these protocols existed:
In the UK there has been a large increase in the number of referrals for children under the age of 12 to the Gender Identity Development Service (GIDS). Historically, pre-pubertal children were supported with a ‘watchful waiting’ approach, with evidence suggesting that approximately 2% to 27% of younger children with Gender Dysphoria were likely to persist with their cross-gender identification following puberty. However, more recently the number of children who persist in their wish to live in their non-assigned gender and who present to the service having already transitioned at home or school, has increased…
Persistence was strongly correlated with the commencement of physical interventions such as the hypothalamic blocker (t=.395, p=.007) and no patient within the sample desisted after having started on the hypothalamic blocker. 90.3% of young people who did not commence the blocker desisted.
Even more clinician-researchers express worry in “Current management of gender identity disorder in childhood and adolescence: guidelines, barriers and areas of controversy”, in Endocrinology, Diabetes and Obesity”:
Hill et al. [17] advocate an affirmative intervention, helping parents to support their child’s declared sex rather than attempting to have the child conform to their natal sex. There is an increasing parental support for young children living as their desired sex; however, desisters may struggle with returning to live as their natal sex when their original desire to live as the opposite sex had been so strongly supported and encouraged by parents and providers, and even accepted by peers.
Other mental and medical health care professionals question the safety of early social transitions, in terms of over-medicalizing an intense, but temporary, psychological condition. In “Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study” the researchers made this observation of socially transitioned girls:
Given our findings that some girls, who were almost (but not even entirely) living as boys in their childhood years, experienced great trouble when they wanted to return to the female gender role, we believe that parents and caregivers should fully realize the unpredictability of their child’s psychosexual outcome…They may help their child to handle their gender variance in a supportive way, but without taking social steps long before puberty, which are hard to reverse.
Some activists argue that the youths described in the above studies were never really “truly trans” and weren’t fully living as the opposite sex. If even these youths with less severe GD had difficulty returning to living as their natural sex, what might be the effect on more seriously dysphoric minors who may come to align with their bodies?
Psychologist Michael Bailey and Eric Vilain (geneticist) add to this discussion in their editorial in LA Times:
For example, the parents of Jazz Jenning, a transgender teen and YouTube celebrity, let their son live as a girl starting at age 5, and all the evidence suggests that she will remain female. The little data we have indicate that parental acquiescence leads to persistence.
A statement from Jack Drescher, MD takes developmental psychology and environmental influences seriously:
What of the gender variant child whose social environment both accepts and encourages an early transition but may be unaware that the child, unwilling to disappoint, has had a change of heart?
Here is a comment from more skeptical and conservative PhDs (Paul W. Hruz, Lawrence S. Mayer, Paul R. McHugh), published, in “The New Atlantis”:
As philosopher Ian Hacking has argued, many psychological conditions are subject to what he calls a “looping effect,” wherein the classification of people as belonging to certain “kinds” can change how those people think of themselves and how they behave.[121] Children and adolescents who are experiencing confusion about gender roles, their sexuality and behavior, and the changes caused by puberty may be especially likely to take up the way of life provided for by a “kind” like “transgender” as a way to make sense of their confusing circumstances, especially when they are subjected to the pressure of being labeled as such by adults in positions of authority, including parents, teachers, psychologists, and physicians.
Other relevant quotes from the same article:
In a 2008 article, the Dutch scientists respond to this concern — the possibility that young adolescents might undergo medical interventions that could ultimately be unnecessary or worse — by arguing that adolescents who continue to identify as the opposite sex and who continue to desire sex reassignment into early puberty rarely come to identify as their biological sex; they also note that none of their own patients who were found eligible for sex reassignment decided against it.[99] But the fact that none of the patients for whom they recommended sex reassignment decided against the procedure may either indicate that their recommendations were based on a sound diagnosis of persistent gender dysphoria, or that their diagnosis — along with the course of treatment that followed from it, including gender-affirmative psychotherapy and puberty suppression — may have solidified the feelings of cross-gender identification in these patients, leading them to commit more strongly to sex reassignment than they might have if they had received a different diagnosis or a different course of treatment…
According to Vilain, physicians are far too willing to recommend social transitions for children. As a result, Vilain believes the vast majority of children currently undergoing social transitions in the U.S. might not actually be transgender and, thus, might not be best served by embracing a sex that doesn't match their gender. ‘If the children are pushed in this belief it will be much much harder for them to get out of this belief because everyone will have agreed on it very, very early on,’ Vilain said. "What worries me is that, indeed, there might be in the upcoming years a considerable number of these children that are placed on a path that we don’t fully know the outcome.
Clinicians with these viewpoints (even when there is data to support them) are censored by WPATH and other transgender organizations. Yet, these groups have so far not offered solid refutation or clear research results to address any of the above concerns.
C. Evidence teenage girls are being put at risk for unnecessary medical body modifications, by gender affirming doctors & therapists; boys may be impacted in other ways
Some youths continue to be dysphoric enough to want to medicalize. At the same time, certainty of transgender identity isn't true for all young people, according to desistance stats and real-world observation. Gender dysphoria in youth (and adults) happens due to a complex set of factors and isn't always something with a clear boundary (just as bisexuality rests between homo and heterosexuality in varying degrees). This is why many gender professionals advocate for a "watchful waiting" model (also called "the Dutch model") rather than a gender-affirmative model.
Previously, most young people seen by gender clinics had early-onset gender dysphoria that began in early childhood. In the past, if these youths remained trans-identified into puberty, they would more likely maintain trans-identification into adulthood. In those cases, one might argue that denying "affirming care" is unethical. Currently, many more female teenagers and young adults are identifying as trans (often out of the blue), drastically changing the demographics of those receiving treatment. This group seems to experience higher rates of desistance and possibly regret. They identify as trans as teenagers but eventually outgrow GD.
Males tend to claim they are transgender at younger ages than females, according to information collected from gender clinics. Because of the shift to an affirmation model, males are more likely to spend much more extended periods in a social transition from a young age. This longer period may ultimately influence their sense of gender identity.
Surgery is being performed on minors in some places (for example the United States), including double mastectomies on females as young as 13 years old (Olson 2018). Hormone blockers (if followed by estrogen) have permanent effects on males (see below). So, the reality that trans identification is not always permanent is pertinent to the discussion of transitioning children and teenagers.
Risks to girls

There are multiple recorded cases of teenage girls (many lesbians, but also bisexual and heterosexual females), who were put at risk of unnecessary medical interventions that would have permanently altered their bodies. Many did not have childhood GD (they presented with the rapid-onset variety discussed in the above desistance section, studied by researcher Lisa Littman). Even though they met the diagnostic criteria for gender dysphoria under DSM-V (persistent for 6 months), they later fully desisted.
Some had gender dysphoria for several of their teenage years and demanded irreversible body modifications (from testosterone use and double mastectomies), but later outgrew these strong, but temporary desires. Some had other serious mental health issues, or a history of sexual abuse or other trauma. In many of these cases, the mental health and medical professionals treating these youths enthusiastically supported their social and medical transitions. It was the parents’ decisions (contrary to therapist or medical advice) to “watch and wait” that protected their children from over-medicalizing what ultimately turned out to be a transient issue.
In addition, some parents, educators, and mental health professionals worry that there’s a social contagion factor influencing some young females. The counter argument to social contagion, is that females often become more dysphoric with the onset of breast development. This may be true, but why have these spikes in dysphoria in puberty not happened in the past?
Some of the increase in trans youth is indeed due to the rise in cultural attention to the issue. However, there are now cases involving females who had very strong feelings of GD that naturally resolved during their tween, teen, or young adult years without surgical or hormonal interventions. Therapists and medical professionals cannot discern these young people from “truly” transgender youth, as many desisters met current GD diagnostic criteria under DSM-V. The mental health and medical community involved in youth transitions should acknowledge this challenge to the public. They are morally obligated to admit that inappropriate transitions are happening.
Currently, and with increased visibility through blogs and videos, young adult females who transitioned as teens and have now detransitioned are adding to these discussions. More cases such as these can be found on 4thwave.now, a site for parents who are primarily liberal-leaning and pro-LGB but are skeptical about the affirmative model. Dr. Littman’s ROGD study and a non-peer-reviewed survey created by a detransitioned lesbian also highlight the reality of desistance, detransition, and regret.
For a full discussion on the increasing numbers of female teenagers identifying as trans see here
Risks to boys
Since there are so many more females identifying as trans and anecdotally, regret rates seem to be going up, people may view inappropriate medical transitions as more of a risk to bisexual, lesbian, and even heterosexual females, than to effeminate young gay males. Desistance happens in dysphoric males as well, as seen in the above data.
One case involves a male who was very dysphoric at 12 years old but outgrew GD two years later at age 14. He now needs breast tissue removal. He met the diagnostic criteria for GD, and a doctor illegally prescribed female hormones through his mother. This boy was never put on blockers. Had his puberty been suppressed early (now common practice), he may not have desisted at all. It’s possible his brain could have been impacted in a way that affected his feelings about his gender due to the prevention of sex hormone exposure.
In the past, more males than females were assessed for GD at very young ages. Some of this was due to parents not being as accepting of gender nonconforming boys as they are of girls and to what Dr. Zucker perceived as parental concern with “proto homosexual” behaviors. However, females seem to identify as trans at slightly older ages, closer to puberty, and in previous studied, they desist less often. This quote is from the researchers Tavistock clinic:
Focussing on all referrals under the age of 12 between 2001 and 2011(Mean age = 10.09), 50% of the cases were persisting in their wish to live in their non-assigned gender post-pubertally (at age 16) and were actively expressing the wish to progress with physical treatments. There was a significant difference in persistence rates between natal sex (t=.548, p<0.001), with 75%NF and 25% NM persisting at age 16.
For this reason, early social transition may be riskier for males due to the longer time spent living in a social transition (and in higher numbers). Steensma et al. (2013), has in fact, shown an association between social transition and persistence. Furthermore, we can't ignore nored that some of these children may be pre-gay males. When puberty is halted at a young age (as young as 11), and social transitions begin as early as 3 years old, it is impossible to know true desistance/persistence rates without a control group.
The affirmative medical transition model for minors may also pose a risk to heterosexual teenage males who have “late-onset”—sometimes called autogynephilic (AGP)—transgenderism. Their dysphoria is related to their sexual orientation and strong emotional need to feel female and be seen as female. Aitken et al. (2013) seems to indicate more of these individuals are identifying as trans at younger ages, according to the sexual orientation data in this study.
There is a concerted effort to discredit the theory of autogynephilia in the trans community. However, there is much evidence for it. Shame around this diagnosis is unnecessary and could harm the quality of therapy for young people with differing types of gender dysphoria
Yet, AGP individuals often make up over 50% of trans-identified males in research cohorts. Most research focused on AGPs involves adults who transitioned in middle age, often after marriages to women and fathering children. Transition occurred after having tried other strategies to cope with GD. Since AGP can present itself on a spectrum of severity (from cross dressing to wanting hormones and bottom surgery), having these young males transition in their teens or early adulthood may increase regret rates.
In summary, the reasons to be concerned that false positives will happen under a gender dysphoria affirmation model are:
1) A small number of adults regret transition (it’s low but they exist, stats range from 1%-20%, but usually under 4% in studies. This indicates perfect screening for children will be impossible.
2) Even some prepubescent children with GD desist.
3) GD can fall on a continuum or be due to complex issues, and predicting outcomes for minors is likely not possible.
4) Demographics are changing, especially with an increase of females and late-onset variety males (AGP) wanting to transition as teens.
5) Social transitions of young children and puberty suppression in tweens may affect outcomes.
6) There is a growing community of detransitioners. Currently, detransitioners report receiving little-to-no clinical support when requesting help with detransition.
Some mental health and medical professionals believe alse positives are necessary collateral damage to support trans-positive healthcare. It is still in the interest of the LGB community to know how often false positives happen. This affects the diversity and well-being of LGB communities and the human rights of gender nonconforming minors (regardless of orientation) with questionable ability to give consent.
D. Hormone blockers may prevent a youth from outgrowing gender dysphoria
Lupron (a GnRH analog also called “hormone/puberty blockers,” Leuprorelin, or Leuprolide) has been used for years as a chemotherapy drug to suppress sex hormones that feed cancerous tumors and to treat precocious puberty in girls, and less commonly in boys. Mental health and medical professionals who support the affirmative model always tout Lupron as “fully reversible.” These include PhDs such as Dr. Olson-Kennedy, Kristina Olson, Diane Ehrensaft, Norman Spack and members of WPATH in general. WPATH justifies this off-label use of Lupron in this quote:
Their use gives adolescents more time to explore their gender nonconformity and other developmental issues; and (ii) their use may facilitate transition [to living as the opposite sex] by preventing the development of sex characteristics that are difficult or impossible to reverse if adolescents continue on to pursue sex reassignment.”
There is no evidence that Lupron is “fully reversible,” or that it doesn’t affect gender identity development, as a study with a control group would be needed to determine this claim. There’s no proof that Lupron doesn’t alter brain development (in fact, there is some evidence that it does) or the physical health of a child.
What is known, is that puberty seems to resume if Lupron is stopped, but that statistically, desistance is almost unheard of in children who had their natal puberty suppressed.
Since no one knows what causes a youth with childhood GD to resolve their dysphoria (usually into puberty), professionals cannot assert that hormone blockers—which affect hormonal exposure to the youth’s brain (hormones that are critical to normal brain development)–won’t alter the gender identity, sexuality, cognitive function, personality, or long-term health of the young person.
Mental health and medical professionals who claim blockers are known to be completely reversible and safe are violating full disclosure and proper informed consent, by withholding important information. Nevertheless, this assertion is made routinely. Medical and mental health communities should be obligated to provide evidence that hormone blockers do not affect the long-term health, psychosexual development, or gender identity outcomes for minors put on hormone blockers since it is becoming the norm to recommend them
No studies have been published that determine why children seldom desist once put on hormone blockers. Gender clinicians also haven’t demonstrated that this lack of desistance is due to a perfectly sound screening process. Moreover, professionals and the media have failed to report on the lack of desistance in children who’ve had their natal puberty suppressed.
Very few children desist once put on hormone blockers
The rates of desistance in children put on hormone blockers is extremely low. In several clinics, the number is zero (see below). It’s reasonable to assume that only the most dysphoric youths are put on blockers, but it may be necessary for a youth to experience some time and perhaps anxiety around puberty to resolve their distress over gender. Lupron may not just block hormonal puberty; its use may also block a process of self-acceptance.
Endocrinologist Norman Spack has a zero desist rate:
Spack has, he says, put “about 200 children” on to hormone blockers at the onset of puberty. Of these, 100% have gone on to take cross-sex hormones because “no one changes their mind”. At which point, I think: no one?
From the VU University Medical Center clinic in Amsterdam:
No adolescent withdrew from puberty suppression, and all started cross-sex hormone treatment, the first step of actual gender reassignment.” These were out of 70 children put on hormone blockers.
Dr. Johanna Olson-Kennedy on desistance post hormone blockers:
It’s incredibly rare. There’s really only one child that has been reported in the literature that went on the blockers and did not go on to cross-sex hormones, or gender-affirming hormones.
And:
You can take them off without any problems or major medical problems. But it’s very rare that that happens. In my practice, I have never had anyone who was put on blockers, that did not want to pursue cross-sex hormone transition at a later point
In clinics with stricter gatekeeping such as those under the Dutch researchers (Steensma et al.), their zero desist rate is possibly due to intense screening and these teens were generally older when they started puberty suppression. These consistently low rates across the board warrant scrutiny because children are put on hormone blockers at younger and younger ages, giving them less time in normal puberty.
Therapists, doctors, & even the Endocrine Society recommend suppressing puberty for dysphoric minors before they may start to align with their natural body
The general consensus among gender dysphoria experts is that if a young child is dysphoric and continues to be so into puberty, they are very likely to transition. Medical professionals, often at the recommendation of mental health professionals, have stopped waiting until a youth has spent any meaningful amount of time in puberty before prescribing hormone blockers or even cross-sex hormones. Early puberty blockade, which suppresses approximately 95% of all sex hormone production, reduces the possibility of exploration during a natural state of growth and development.
There are now multiple examples of children being put on blockers as young as age 10 (one famous “trans kid” celebrity, Jazz Jennings, who socially transitioned as a young child had puberty suppressed at age 11 and began cross-sex hormones at age 12). A few more examples are below:
A dysphoric male was puberty suppressed at age 11 in California.
Here Johanna Olson Kennedy admits to blocking a 9-year-old (Gender Odyssey 2017):
I had another, started testosterone at thirteen, discontinued both and was starting to go through puberty and now was like, aahhh I gotta get back on T and went through “I’m non-binary,” assigned female at birth, blocked at nine.
The Endocrine Society has recently changed its guidelines to lower the ages the administer medical treatments. They seem unconcerned with reports that letting children experience some puberty often leads to desistance. They suggest starting puberty blockers for transgender children at a stage of development known as Tanner stage 2, which is 9-11 years for a girl and 10-12 years for a boy. These youths will spend no time in Tanner 2 or later stages of natal puberty.
Why is this concerning? Dr. James Barrett, a psychiatrist at the Charing Cross clinic, the oldest gender identity clinic in Britain said:
If you wait until puberty has got a little way along, a fair proportion of the children change the clinical presentation and feel more like a straightforward lesbian and gay kid.They don’t seek social role change anymore and will end up with no need for lifelong medical intervention, surgery and no loss of fertility should they want children.
The clinicians in the Netherlands state that complicated factors during adolescence help the child to better understand themselves:
It is recommended to specifically address the adolescents’ feelings regarding the factors that came up as relevant in our interviews (i.e. the effects of the changing social environment, the response to anticipated or actual puberty, and the emerging romantic/sexual feelings and sexual partner choice), before any medical steps are taken (e.g. to suppress further pubertal development).
Therapists and doctors do not know if puberty suppression interferes with this process. They are preventing the flush of testosterone or estrogen in these children’s bodies and brains, not knowing if these hormones are a part of why a youth may outgrow GD. This practice is marketed to the public as wholly reversible and safe, with no controls or evidence to validate those statements in relation to psychological effects.
Furthermore, it may violate the AMA’s code of ethics of informed consent to promote puberty suppression as reversible when the psychological effects on gender identity are entirely unknown. These factors also have to be considered and weighed against the arguments for implementing life-changing protocols for dysphoric youth. Lack of full disclosure has led to malpractice lawsuits. From the AMA’s code of medical ethics:
Withholding information without the patient’s knowledge or consent is ethically unacceptable... “full disclosure of possible side effects is required by the ethical norms of respect for persons and informed consent.”
E. Three anecdotal examples the affirmative model may increase persistence
Steensma et al (2013) showed significantly higher rates of persistence in socially transitioned children, which suggests the possibility that social transition fails to provide the support needed for pre-gay and lesbian youths to adjust to their sexed bodies naturally.
Since there are no control groups and no plans for studies that include youth supported in their gender nonconformity but not in complete social transition, we provide three examples below that an affirmative model may increase GD persistence. James Cantor, the PhD cited in desistance research above, had a Facebook exchange with WPATH members and affirmative model advocates. Jenn Burleton, a very politicized trans activist, reports a zero-desistance rate in a US clinic. A zero desist rate is previously unheard of in the research:
The below screen shot is an excerpt from a court case in Australia discussing desistance in an affirmative model clinic. The desistance rate under this affirmation protocol is only 4% and becomes zero once puberty is suppressed:
Almost all youths put on hormone blockers go on to medically transition in more recent studies.
It appears likely that complete social transition supported by parents and pro-transition gender clinics may increase persistence.
Transgendertrend reports that during the seminar“Gender Non-Conforming Children: Treatment Dilemmas In Puberty Suppression,” Dr. Bernadette Wren, head of Psychology, Gender Identity Development Service at the Tavistock & Portman NHS Foundation Trust stated that 12- 27% of ‘gender variant’ children persist in gender dysphoria; that percentage rises to 40% among those who visit gender clinics. If these numbers are accurate, there is a significant increase in persistence when children are cared for under a gender identity-affirming protocol.
The above examples point to zero or significantly lowered desistance rates, which contradict earlier data, yet they provide no information to explain this shift. They provide no evidence their screening process is more thorough in comparison to past studies. And there have been no public comments from gender clinicians to indicate they plan to do so.
F. Conclusion, desistance
Although early social transitions and prescribing puberty suppressants at the onset of puberty is very possibly going to prevent some youth from resolving their GD naturally, some studies and observations do demonstrate positive outcomes for dysphoric youth socially transitioned and put on hormone blockers (Steensma et al (2013), (Olson 2016), Norman Spack Ted Talk).
The results of these studies are the reason why this protocol has been adopted so quickly by parents, schools, mental health, and medical providers, as trans youth and adults are an at-risk population for mental illness and suicide. But there should be much greater effort to more fully and accurately weigh the cost/benefits and risks to borderline youth, something that currently appears to be a low priority among the health professions generally.
The argument is denying “affirmative care” in unethical. But prioritizing care that over-medicalizes youth also creates an ethical problem and inflicts medical damage on all youth (see Topic #2). Initiating hormonal interventions which will affect these young people for their entire lifetime, not just their childhood, could lead to greater harm then employing watchful waiting that is supportive of gender nonconformity.
There are attempts to find more concrete proof of "truely trans” in brain structure research. For example, one study shows that there may be brain structure differences between trans individuals and homosexuals, who are the at-risk population for inappropriate transition as minors:
While this study is interesting, there is also evidence that gender dysphoria is much more complicated and the difference between “trans kids” and borderline dysphoric GD LGB youth (or heterosexual female adolescents, in some cases) start in-utero or are the result of other biological effects on a continuum where culture and environment may also play a major role.
For example, Ray Blanchard has shown an effect of birth order and older brothers in the prevalence of male homosexuality related to inborn effects on fetal brains. This association has now been found in dysphoric males, complicating the concept that there is always a clear distinction between homosexuality and transgender identities. Also, while biology is important in determining human behavior in general, recent research which found brain differences like the above study (on adults) may also be due to environmental factors (at least partially) and not to hard wired biological make-up. It is very unlikely doctors will ever be able to do brain scans on growing minors to determine the differences between desisters and persister (more on nature verse nurture in Topic #10)
James Cantor, a sexologist and University of Toronto professor, comments on the reality of desistance of gender dysphoria in minors:
The state of the science is made clear simply by listing the results of the studies on the topic (desistence of youth GD). Despite coming from a variety of countries and from a variety of labs, using a variety of methods, all spanning four decades, every single study without exception has come to the identical conclusion.
He makes a balanced statement here:
Importantly, these results should not be exaggerated in the other direction either: The correct answer is neither 0% nor 100%. Although the majority of transgender kids desist, it is not a large majority. A very substantial proportion do indeed want to transition as they get older, and we need to ensure they receive the support they will need. Despite loud, confident protestations of extremists, the science shows very clearly and very consistently that we cannot take either outcome for granted.
Affirmative model advocates now argue against desistance research claiming it is “transphobic” but they have no hard evidence to back up their assertions. As a result, youth are being transitioned based on unfalsifiable data.
© Gender Health Query, 6/1/2019
References for Topic 1
Updates Topic 1
Continue to Topic 2:
Hormone blockers, trans youth, & permanent side effects such as sterility & loss of sexual function
Contents
1) Do children outgrow gender dysphoria?
A. Changes to DSM-V childhood & adolescent dysphoria
B. Desistance / persistence statistics & the association with adult LGB identity
-Desistance stats breakdown of DSM positive children
-Will living full-time as the opposite sex & early hormone blocker use prevent desistance?
-New information on desistance in later onset gender dysphoria (ROGD) mostly in females
-Risks to girl
-Risks to boys
D. Hormone blockers may prevent a youth from outgrowing gender dysphoria
-Very few children desist once put on hormone blockers
E. Three anecdotal examples the affirmative model increases persistence
F. Conclusion, desistance
Back to Outline
More
1. Do they Outgrow Gender Dysphoria?
3. Are children & teens old enough to give consent?
4. Comments safety / desistance unknown
5. Gender dysphoria affirmative model
6. Minors transitioned without any psychological assessments
8. Regret rates & long term mental health
11. Why are so many females coming out as trans / nonbinary?
13. Why is gender ideology being prioritized in educational settings?
14. Problems with a politicized climate (censorship, etc)